- Visibility 275 Views
- Downloads 34 Downloads
- DOI 10.18231/j.ijcap.2024.046
-
CrossMark

Weights of tensor, abductor and adductor muscles of the human larynx
- Author Details:
-
 Mohini Madhukarrao Joshi *
Mohini Madhukarrao Joshi *
-
S. D. Joshi
-
S. S. Joshi
-
Sandeep Pakhale
Introduction
The larynx, which is an air passage is a sphincter device and an organ of phonation and extends from tongue to trachea. The larynx during its evolution has developed a complex mechanism of skeletal structures and neuro-muscular control which allows it to modify the expiratory stream to produce highly complex patterns of sound with varying loudness, frequency and duration.[1] A large number of muscles must coordinate and co-operate smoothly for the efficient production of speech. The accurate co-operation and control of all the different muscles used in speech make it one of the most complex and skilled movements of which man is capable of and it is difficult to acquire and is readily derranged.[2]
From embryologic, anatomic, physiologic and surgical standpoints, the larynx is one of the complex organs of human body. The numerous cartilages, membranes and muscles of the larynx and the singular hyoid bone are covered with mucosa and connective tissue, forming an organ that at first inspection appears deceptively simple. All these parts function as an integral unit that co-operates beautifully with the cerebral hemispheres in the production of speech and regulation of respiration and deglutition.[3] Muscles of larynx can be divided into intrinsic and extrinsic muscles. The extrinsic muscles of the larynx connect the laryngeal cartilages to the hyoid bone above and trachea below. The intrinsic muscles of the larynx interconnect the laryngeal cartilages and help in their mobility Intrinsic muscles of larynx may be divided into: Those that open the glottis: Posterior cricoarytenoid muscle
Those that close the glottis: Lateral cricoarytenoid, thyroarytenoid.
Those that control the tension of vocal ligaments: Thyroarytenoids, vocalis and cricothyroids.
Those that alter the shape of the inlet of the larynx: Aryepiglotticus and the thyroepiglotticus & oblique arytenoids.[4]
In 1881 sir Felix Simon published results of clinical observations of laryngeal palsies which later become embodied in the well known Simon’s law. This states that in a partial laryngeal palsies the abductor muscles are more susceptible to trauma than adductor muscles.[5] The weight of abductor muscle is not more than 25% than adductors which may explain the greater vulnerability of abductors in the event of partial injury the recurrent laryngeal nerve.[5] With this background this was an attempt to measure the weight of cricothyroid (Tensor), posterior cricoarytenoid (Abductor) and lateral cricoarytenoid (Adductor) muscles of the human larynx of regional population.
Materials and Methods
The present study was carried out in the department of Anatomy of a medical university teaching hospital. We used donated and unclaimed dead bodies for the purpose of medical education and research including anatomical examination under the Bombay Anatomical Act 1949. The study was approved by institutional Ethical Committee. The study was carried out on 50 Laryngeal preparations from cadavers. Any cadaver with the possibility of laryngeal damage as a result of disease, diagnostic procedures or surgical manipulation was excluded from the study. The anterior neck was exposed by midline incision and the dissection extended laterally to the angle of mandible superiorly, and along the clavicle inferiorly. After the visualizing the laryngeal prominence of the thyroid cartilage, the strap muscles were resected. Dissection was carried out with the help of dissecting instruments.
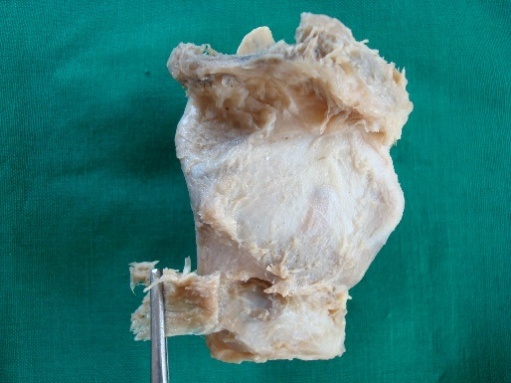
Along with the tongue, the specimen of the larynx was removed by cutting the muscles of soft palate, muscles of posterior pharyngeal wall & fascia. Larynx was separated from tongue from the level of hyoid bone to 3rd tracheal ring. Dissection was carried out with the help of hand lens, dissecting microscope & dissecting instruments. Removal of cricothyroid muscle: The initial step was removal of thin layer of overlying fascia until the muscle fibers were completely exposed ([Figure 1]).
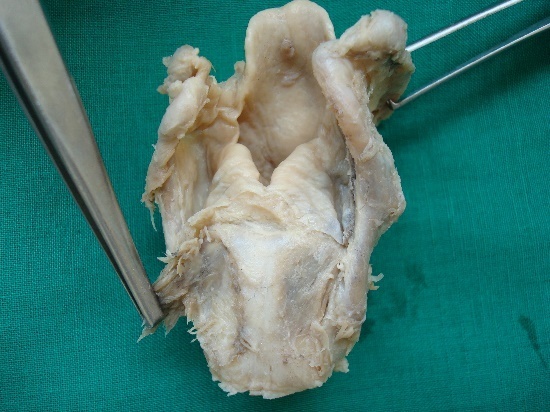
Removal of posterior cricoarytenoid muscle
Posterior pharyngeal wall was cut in the midline. The mucous membrane from the posterior surface of the arytenoid & cricoid cartilages was striped. A thin layer of overlying fascia was removed until the muscle fibers were completely exposed ([Figure 2]).
Disarticulation of cricothyroid joint
Cricothyroid joint was disarticulated by separating the lower part of the lamina of cricoid cartilage & inferior horn of thyroid cartilage with the help of stab knife ([Figure 3]).

Identification and removal of lateral cricoarytenoid muscle
Lateral cricoarytenoid muscle; which was deep to the posterior part of thyroid cartilage, inferior to thyroarytenoid muscle was removed with the help of curved knife ([Figure 4]).

After removal of each muscle it was kept on blotting paper after removal of all moisture and the muscles were weighed on Single pan electronic balance (Shimadzu BL series 2204): (sensitive to 0.01 gm) ([Figure 5]).

Statistical analysis
For weight of each of the muscles, the mean, standard deviation (S.D.) and range (minimum value-maximum value) was calculated. Z test was used to test significance of difference between the two mean.
Results
|
|
Parameter |
Right side Mean ±S.D(mg) |
Left side Mean ±S.D(mg) |
‘Z’ value |
p-value |
Result |
|
1 |
Cricothyroid (CT) |
309.68±102.94 |
332.81±116.7 |
0.04 |
>0.05 |
not significant |
|
2 |
Posterior cricoarytenoid (PCA) |
230.01±60.93 |
231.06±61.35 |
0.007 |
>0.05 |
not significant |
|
3 |
Lateral cricoarytenoid (LCA) |
60.56±24.10 |
63.48±19.67 |
0.15 |
>0.05 |
not significant |
Wide individual variation in weight of the muscles was observed. The Mean weight of the cricothyroid muscle (tensor) was more than the Posterior cricoarytenoid (abductor) & Lateral cricoarytenoid muscle (adductor). The Mean weight of the posterior cricoarytenoid (abductor) was more as compared to Lateral cricoarytenoid muscle (adductor).
Discussion
In present study wide individual variation in weight of the muscles was observed ([Table 1]). The average weight of the cricothyroid muscle (tensor) was more than the Posterior cricoarytenoid (abductor) & Lateral cricoarytenoid muscle (adductor). The average weight of the Posterior cricoarytenoid (abductor) was more as compared to Lateral cricoarytenoid muscle (adductor). The values clearly indicate that cricothyroid (Tensor) is much heavier than other muscles and could be accounted for the fact that, acting either ways it has to move the two heavier cartilages (thyroid & cricoid) covered by all the soft tissues. Secondly the abductor (posterior cricoarytenoid) is solely responsible for the movement of arytenoid, and hence acting from a strong base of posterior surface of lamina of cricoid it has to pull & rotate arytenoid. Whereas, the lateral cricoarytenoid is assisted by other adductors, therefore amongst these three it has the least weight.
The work of Bowden & Sheuer reported that the weight of the abductor muscles of the larynx is not more than 25% of that of the adductors, which may explain the greater vulnerability of the abductors in the event of partial injury to the recurrent laryngeal nerve.[6] The findings of present work are in agreement with those described by Bowden et al.
In a study of the intrinsic muscles of larynx of 54 postmortem larynx, it was observed that while no significant alterations had occurred in cricothyroid, interarytenoid, lateral cricoarytenoid or thyroarytenoid muscles, all the larynges from patients 13 years old or over revealed microscopic changes in the posterior cricoarytenoid muscle, and in many of those from patients over 46 years old there had also been some necrosis and associated reactive changes to this. Posterior cricoarytenoid is the sole abductor of vocal folds, the changes may be a manifestation of continuous activity of this muscle.[7] The changes start with the deposition of coarse lipofuscin granules near the sarcolemma. similar granules are found in the tongue muscle and myocardial fibers from an early age. Only in the posterior cricoarytenoid muscle, however, does concomitant muscle and other sarcoplastic change take place.[7]
Semon states
'The occurrence of an isolated paralysis of the abductor filaments of the recurrent nerve in cases in which the roots or trunks of the spinal accessory, pneumogastric and recurrent nerves are injured or diseased, is not an isolated pathological curiosity. There is a distinct proclivity of the abductor fibers to become affected, in such cases, either at an earlier period than the abductor fibers, or even exclusively.[8] This study of the laryngeal myology is also of special pathological interest, chiefly with regard to problems of nervous lesions. Physiologists and laryngologists are at variance with one another as to the true' explanation of Rosenbach-Semon's law. The following points in connection with the biological constitution of the muscles and the myology of the larynx are noteworthy: (1) The preponderance of sphincter-fibres over dilator fibres. (2) Taking the muscles as special and individual muscles, as it is generally done, there is no muscle containing exclusively dilator-fibres. (3) The Crico-arytaenoideus posticus acting with the Cricoarytaenoideus lateralis, & must cause an approximation of the cords, i.e., act as sphincter. (4) The close connection between the crico-thyreoideus (anticus) and the mass of the Thyreo-arytaenoideus and crico-arytaenoideus lateralis.
According to their main actions, the laryngeal musculature may be divided into three functional groups: (i) muscles varying the rima glottidis (which may be subdivided into constrictors and a singular dilatator); (ii) muscles regulating tension in the vocal ligaments; and (iii) muscles modifying the laryngeal inlet (the so-called ‘sphincter aditus’).[9], [10] Following the traditional description given by Clara,[11] in mammals the laryngeal muscles phylogenetically are derived from two sources: the so-called ‘internal sphincter’, which gives rise to the internal laryngeal muscle, and the external sphincter from which the external laryngeal muscle (cricothyroid muscle) together with the pharyngeal constrictors are derived. According to this scheme, both groups of muscles receive their motor innervation from different nerves, all of them branching off from the cervical part of the vagus nerve.[11]
Burger states that nerve supply of adductors is both recurrent and superior laryngeal.[12] Ziegelman has confirmed by dissections the findings of other anatomists, that internal laryngeal nerve sends branches and communicate with recurrent laryngeal nerve and that contrary to the usual teaching in most instances the arytenoid muscle is supplied by superior laryngeal nerve.[13] Semon should be recognized as a pioneer in the field of neurolaryngology for his research. One of his major discoveries was to identify the localization of cortical and subcortical centers of the motor innervation of the larynx.[14]
Neuromuscular spindles have been demonstrated in all the muscles of the human larynx.
Certain other types of nerve endings, claw ending, and a spiral ending are recorded.
The question as to the significance of the sizes of muscular nerve fibres and of the size-frequency distribution of the fibres is discussed.[15]
Conclusion
This study provides a comprehensive and detailed description of weights of tensor, abductor and adductor muscles of the human larynx from a local population in Western India. Knowledge of such measurements is of fundamental importance for clinical practice in order to prevent unnecessary injury to the larynx. This study of the laryngeal muscles weight is also of special pathological interest, chiefly with regard to problems of nervous lesions.
Ethical Approval
PMT/RMC/2007/.
Source of Funding
None.
Conflict of Interest
The authors declare no conflict of interest.
References
- P Williams, H Bannister, M Berry, M Dyson, P Collins. . Gray’s Anatomy 1995. [Google Scholar]
- WJ Hamilton. . Textbook of Human Anatomy 1976. [Google Scholar]
- JE Skandalakis, JE Skandalakis, GL Colborn. . Skandalakis' Surgical Anatomy: The Embryologic and Anatomic Basis of Modern Surgery 2004. [Google Scholar]
- N Weir. Anatomy of the larynx and tracheobronchial tree. Scott-Brown’s Otolaryngology 1987. [Google Scholar]
- F Semon. Clinical remarks on the proclivity of the abductor fibres of the recurrent laryngeal nerve to become affected sooner than the adductor fibres, or even exclusively, in cases of undoubted central or peripheral injury or disease of the roots or trunks of the pneumogastric, spinal accessory, or recurrent nerves. Arch Laryng 1881. [Google Scholar]
- REM Bowden, JL Scheuer. Weights of Abductor and Adductor Muscles of the Human Larynx. J Laryngol Otol 1960. [Google Scholar]
- GM Guindi, L Michaels, R Bannister, W Gibson. Pathology of the intrinsic muscles of the larynx. Clin Otolaryngol Allied Sci 1981. [Google Scholar]
- JA Kirchner. Simon’s law a century later. J Laryngol Otol 1982. [Google Scholar]
- LH Bannister, R Parker, J Joseph, PL Williams, LH Bannister, MM Berry, P Collins, M Dyson, JE Dussek. Respiratory system. Gray’s anatomy 1995. [Google Scholar]
- VE Negus. . The comparative anatomy and physiology of the larynx 1949. [Google Scholar]
- M Clara. . Das Nervensystem des Menschen 1953. [Google Scholar]
- H Burger. Associated paralyses of the vocal cord. J Laryngol Otol 1934. [Google Scholar]
- EF Ziegelman. Laryngeal Nerves. Arch Otolaryn 1933. [Google Scholar]
- J Kuczkowski, L Plichta, C Stankiewicz. Sir Felix Semon (1849-1921): pioneer in neurolaryngology. J Voice 2012. [Google Scholar]
- MFL Keene. Muscle sphindles in human laryngeal muscles. J Anat 1957. [Google Scholar]