Introduction
Diabetes mellitus(DM) refers to a group of common metabolic disorders that share the phenotype of hyperglycaemia.1 These metabolic disorders share the common feature of hyperglycaemia caused by defects in insulin secretion, defect in insulin action or, most commonly both.2 Today, more than half a billion people are living with diabetes worldwide. Causative factor for diabetes is many.1 Diabetes mellitus is caused by a complex interaction of genetics and environmental factor. Factors contributing to hyperglycaemia include reduced insulin secretion, decreased glucose utilization, and increased glucose production.1 Increasing sedentary lifestyles and poor eating habits have contributed to the simultaneous escalation of T2DM and obesity, which some have called the diabesity epidemic.2 Diabetes mellitus is classified on the basis of the pathogenic process leading to hyperglycaemia into two broad categories, designated as either type 1 or type 2 DM. Type 1 diabetes (T1D) is an autoimmune disease characterized by pancreatic β-cell destruction and an absolute deficiency of insulin. It accounts for approximately 5% to 10% of diabetes and is the most common subtype diagnosed in patients younger than 20 years of age.2 Type 2 diabetes (T2D) is a heterogeneous group of disease caused by a combination of peripheral resistance to insulin action and a secretory response by pancreatic β cells that is inadequate to overcome insulin resistance (“relative insulin deficiency”). It characterized by variable degrees of insulin resistance, impaired insulin secretion, and increased hepatic glucose production. Approximately 90% to 95% of diabetes patients have T2D.3 Vast majority of individuals with type 2 diabetes mellitus is overweight. Both type 1 and type 2 are preceded by a period of progressive worsening of glucose homeostasis, followed by the development of hyperglycaemia that exceeds the threshold for clinical diagnosis.1 In terms of type 2 diabetes, this phase is referred to as prediabetes and are more specifically classified as impaired fasting glucose (IFG) or impaired glucose tolerance (IGT).1 Although type 2 DM more typically develops with increasing age, it is now being diagnosed more frequently in children and young adults, particularly in obese adolescents.1
In patients with diabetes, vascular complication is the main reason for the impaired life expectancy. Diabetic nephropathy and retinopathy are the largest contributors of end stage renal disease and blindness. Vascular manifestation of the disease is the most serious manifestation of the disease.4 Persistent inadequate control of blood glucose level over time may alter regulation of inflammatory pathways that are involved in the impairment of lung function. The abundance of extensive connective tissue in lung raises the possibly that the lung as a target organ for diabetes. The effect of diabetes on nervous system, cardiovascular system, renal system, immune system, are studied widely. Study on pulmonary manifestation of diabetes need much more attention, especially in India, as a large proportion of Indian population have impaired pulmonary function and has diabetes as co morbidity. Association of diabetes and pulmonary function especially with that of duration of diabetes need to be studied deeply. Several studies and theories explain relationship of glycosylation and oxidative stress with impaired cross linkage of connective tissue 6 and thus lose their elasticity and strength.5 Even though the association between diabetes and lung function has been described, its clinical significance is not yet been studied deeply.5 Recently some studies shown some relation of alteration of pulmonary functions in inadequately blood glucose controlled diabetic patients. There are large lacunae in terms of studies from India which look into the association of pulmonary function in patients with diabetes mellitus.6 Such kind of studies are limited as Kerala is concerned. Through this cross-sectional study, I tried to find out whether there is any association of pulmonary dysfunction and diabetes and to look for any pulmonary function abnormality in diabetic patients.
Relevance of the Study
The World Health Organization estimates that more than 180 million people worldwide have diabetes, and by 2030 it is expected that this number will have doubled.4
In a recent study estimate that the cumulative incidence of T2DM in Kerala is 21.9% and the incidence of prediabetes is 36.7%.7 As the prevalence of diabetes in our state continuously rises, the complication related to it also will peaks up in near future.
When coming to the complications of diabetics, mostly till now we were focussing on diabetic neuropathy, nephropathy and retinopathy, least studied are the pulmonary complications.
It is not clear whether inadequate glucose control in type 2 diabetes mellitus is associated with impaired pulmonary functions. Hence, this study will be done to assess pulmonary function in type 2 diabetes mellitus along with duration of diabetes in northern part of Kerala, and this helps in creating awareness for adequate control of blood glucose among people so as to prevent pulmonary complications in them.
Aim
To evaluate the pulmonary function tests in type 2 diabetes mellitus and their correlation with glycaemic control.
Materials and Methods
Study population
Includes type 2 diabetes patients attending medical OPD or admitted in medical ward and willing to participate in the study.
Inclusion criteria
All patients with type 2 diabetes mellitus in the age group of 30-50 years belonging to either sex attending OPD and admitted in medical wards.
Exclusion criteria
Smokers8
Pregnancy
Body mass index >309
History of Acute Respiratory Infections in previous 3 months.
Known case of Cardiovascular disease, Chronic Obstructive Pulmonary Disease, bronchial asthma, Pulmonary Tuberculosis, Interstitial Lung Disease, lung cancers.
Known case of previously diagnosed rheumatoid arthritis/collagen vascular diseases.
Patients with chest wall deformity affecting pulmonary function tests.
Deranged renal function, serum creatine > 1.5.
Uncontrolled systemic hypertension with drugs.
Sample size estimation
Formula for difference in means was used for sample size calculation
Where the level of significance is taken as 5%, Z1-α/2= 1.196 and Z 1-β/2 correspond to a power of 80% i.e., 0.84 and μd2 is 19.9.
The sample size is 20 in each group and I intend to conduct the study for 30 persons for each group.2
Study procedure
All subjects included in the study underwent following investigations and relevant history taking.
Fasting blood sugar, Post prandial blood sugar, HbAIc.
Pulmonary function tests- Tidal volume (TV) (normal:500 ml), Inspiratory reserve volume (IRV) (normal: : 3000 mL) Expiratory reserve volume (ERV)(normal: 1100 mL), Forced Vital Capacity (FVC)(normal : 4600 mL) Forced expiratory volume in 1 second (FEV1)(normal : > 80% of FVC) FEV1/FVC : 0.75 – 0.80 peak expiratory flow rate (PEFR) (normal : 400 to 600 L/min).10
Participants were grouped as controlled diabetic or uncontrolled diabetic based on American Diabetes Association criteria,11
Patient were classified into group A and group B based on their glycaemic control.
Group A: Patients of type 2 diabetes with good glycaemic control that is HbA1c</=6.5.
Group B: Patients of type 2 diabetes with poor glycaemic control that is HbA1c>6.5.
All patients PFT was done.
Result
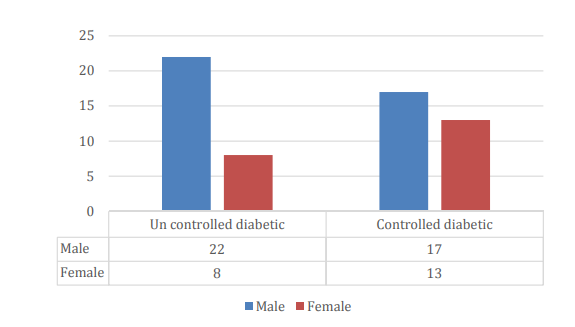
Our study population contains 60 patients of which 30 are diabetic with good glycaemic control and 30 with poor glycaemic control. Average FBS, PPBS, and HbA1c among controlled diabetic was found to be 92.3, 119.7 and 5.9 respectively whereas average value of FBS, PPBS, and HbA1c in uncontrolled diabetic group was found to be 118.6, 173.9 and 7.69 respectively. In our study population, 37% are uncontrolled diabetic males, 28% are controlled diabetic males, 13% are uncontrolled diabetic females and 22% are controlled diabetic females.
Pulmonary testing in study population
60% of uncontrolled diabetic people had reduced FVC compared to 33.33% percentage of controlled diabetic having reduced FVC.
18 out of 30 uncontrolled diabetic patients have reduced FVC and 10 out of 30 controlled diabetics has reduced FVC.
In uncontrolled diabetic individuals, out of 22 males, 13 has got reduced FVC and out of 8 uncontrolled diabetic females, 5 of them have reduced FVC. In case of controlled diabetic individuals out of 17 males, 5 of them have reduced FVC and among 13 controlled diabetic females, 5 of them have reduced FVC.
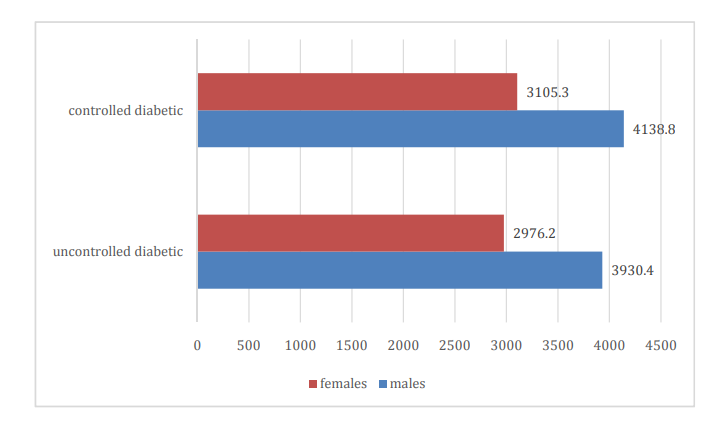
The average FVC among uncontrolled diabetic males was found to be 3930.4 and that for females was found to be 2976.2. The average FVC among controlled diabetic males was found to be 4138.8 and that for females was found to be 3105.3.
The average FEV1/FVC % of uncontrolled diabetic males was 78%, that of uncontrolled diabetic females was 77%. Average FEV1 % in controlled diabetic males was 79.8% and controlled diabetic females was 78.6%.
The average FEV1 of uncontrolled diabetic males was found to be 3075.4 and that of uncontrolled diabetic female was found to be 2315.5. The average FEV1 value of controlled diabetic males was 3304.9 and that of controlled diabetic females was 2440.8.
PEFR among controlled diabetic males were found to be 601.17 and that of females was 446.15. In case of uncontrolled diabetic individuals, average PEFR was found to be 579.09 and that of uncontrolled diabetic females were found to be 391.25.
Pulmonary function test and HbA1c correlation
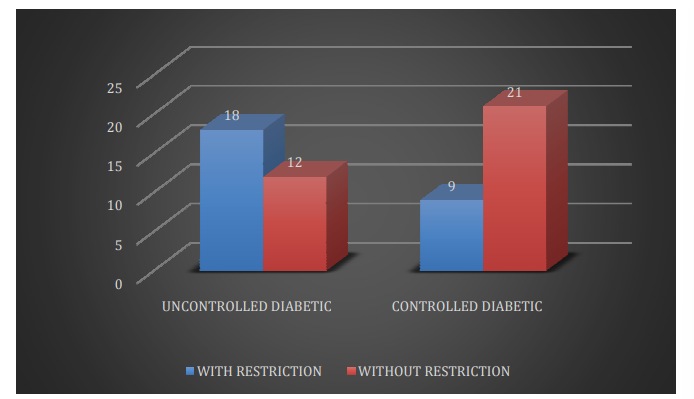
Out of 30 uncontrolled diabetic individuals 18 people has restriction in lungs and 12 without restriction. In case of controlled diabetic individuals, out of 30 individuals only 9 were having restriction and 21 without restriction.
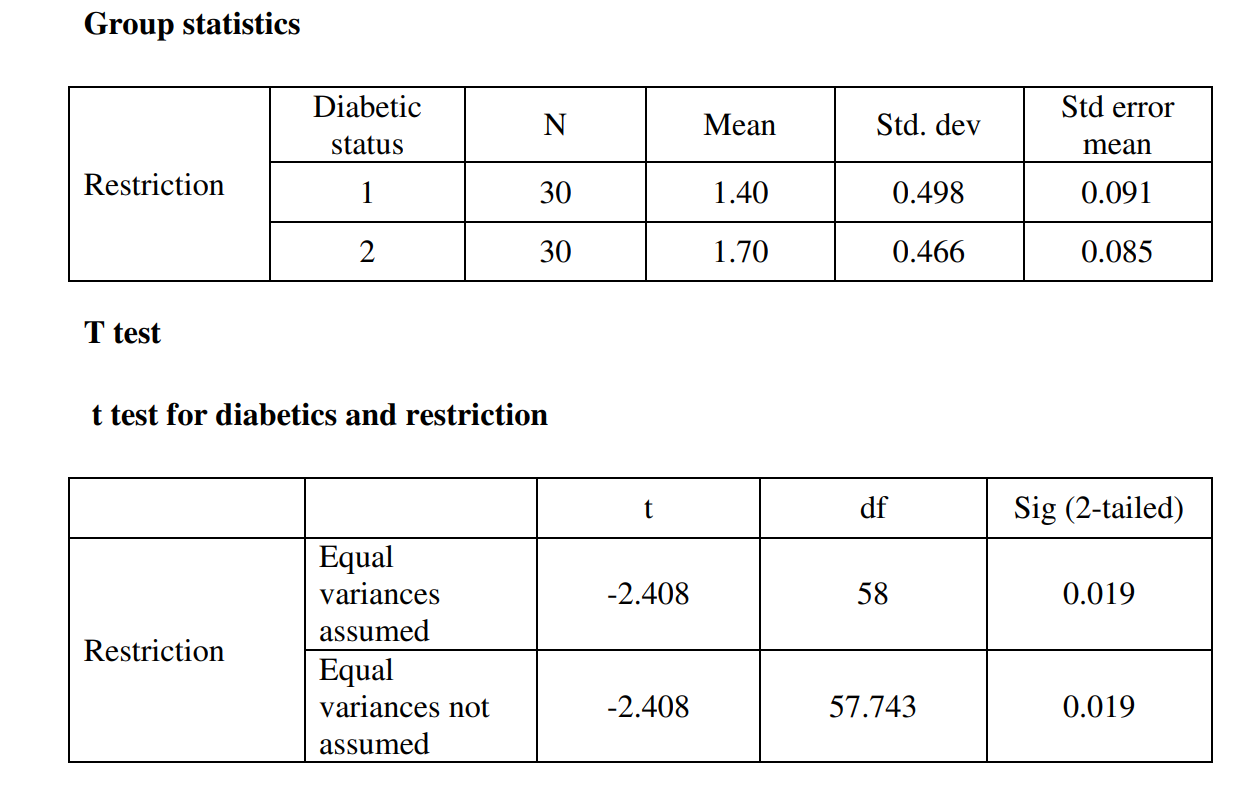
Around 60% of the uncontrolled diabetic people was having a restrictive type of lung dysfunction when compared to 30% in controlled diabetics with a p- value of 0.019 (p value).
Conclusion
In the study we could found out that 18 out of 30 uncontrolled diabetic patients showed a reduced FVC. This shows that about 60% of the uncontrolled diabetic patients showed a reduced FVC in comparison with 30% of controlled diabetics having reduced FVC. The average FVC among uncontrolled diabetic males in our study was 3930.45 ml in contrary to 4138.82 ml in controlled diabetic males, also average FVC in uncontrolled diabetic females in our study was 2976.25ml in contrary to 3105.38 ml in controlled diabetic females. This strongly suggest a restrictive type of lung pathology in the uncontrolled diabetic individuals.
We also found the FEV1 values of lung in both uncontrolled diabetic and controlled diabetic individuals. FEV1 values were found to be slightly decreased in uncontrolled diabetic when compared to controlled diabetic counterparts. The average FEV1 of uncontrolled diabetic males was found to be 3075.4 and that of uncontrolled diabetic female was found to be 2315.5. The average FEV1 value of controlled diabetic males was 3304.9 and that of controlled diabetic females was 2440.8. 67 The average FEV1/FVC % of uncontrolled diabetic males was 78%, that of uncontrolled diabetic females was 77%.
Average FEV1 % in controlled diabetic males was 79.8% and controlled diabetic females was 78.6%. A reduced FVC and a preserved FEV1/FVC, suggests a restrictive type of lung dysfunction. So, we grouped all the individuals into two class, that is one who with restrictive type of lung dysfunction and one without.
A comparison of lung restriction was done between uncontrolled diabetic and controlled diabetic. It was found that, out of 30 uncontrolled diabetic individuals, 18 people have restrictive lung dysfunction and 12 without. In case of controlled diabetic individuals, out of 30 individuals only 9 were having lung restriction and 21 without restriction. It was found that 60% of the uncontrolled diabetic people was having a restrictive lung dysfunction when compared to only 30% of controlled diabetic having restriction in lungs. When comparing restrictictive lung dysfunction in uncontrolled diabetic and controlled diabetics with independent t test, this was found to be significant with a p- value of 0.019(p value < 0.05 was considered significant at 95% confident interval). These results clearly indicates that in our study, the uncontrolled diabetic individuals are having a significant restrictive type of lung pathology when compared to their controlled diabetic counterparts.
We also found out that in our study there was a slight decrease in PEFR values. The average PEFR among controlled diabetic males were found to be 601.17 and that of females was 446.15. Average PEFR among uncontrolled diabetic males was found to be 579.09 and that of uncontrolled diabetic females were found to be 391.25. PEFR values are decreased in many lung diseases including restrictive type of lung dysfunction but it is significantly reduced in obstructive type of lung disease
Diabetes is a very common and important comorbidity in people. It is associated with many complications affecting many systems that includes renal system, nervous system, vascular system, respiratory system. It affects respiratory system in many ways. From our study it is seen that uncontrolled diabetes causes reduction in FVC and a preserved FEV1/FVC ratio, which suggest a restrictive type of dysfunction in their lungs. It is also seen that duration of diabetes is also an important factor in the pathogenesis of the restrictive lung dysfunction.
The prevalence of some microvascular complications is two-to-three-fold higher in youth with type 2 diabetes than those with type 1 diabetes of a similar age.4, 12 The presence of advanced complications during the most productive time of life affects the patient’s personal life, professional life and impose them with huge financial burden for the treatment.
So, it is recommended that all diabetic patients need to make sure that their blood sugar levels are adequately controlled so as to avoid complications associated with diabetes. All the diabetic patients especially those who have a long history of diabetes need to check their pulmonary function tests on a timely basis to avoid pulmonary complications of diabetes.
Also, a healthy diet, regular physical activity, maintaining a normal body weight and avoiding tobacco usage are proven ways to prevent or delay the onset of type 2 diabetes and its complications. Breathing and aerobic exercises can be done to increase once lung health. These life style modifications which are proven to delay diabetes or their complications are to be given much more importance.
Limitations of the Study
Static lung volumes of lung could not be measured as the spirometry in our clinics do not measure values like TV, IRV, ERV etc.
Due to prevailing Covid 19 situation during the study period, available study population was limited, so to meet the sample size some individuals couldn’t met the criteria of BMI.