- Visibility 168 Views
- Downloads 18 Downloads
- DOI 10.18231/j.ijcap.2023.010
-
CrossMark

Morphological study of glenoid cavity of scapula
- Author Details:
-
 Mohini Joshi *
Mohini Joshi *
-
Sandeep V Pakhale
Introduction
The scapula is a big, flat, triangular bone that extends from the second to the seventh ribs on the posterolateral side of the chest wall. The glenoid cavity that joins the scapula is truncated and large, and it can be regarded as the scapula's head.[1] The morphology of the glenoid cavity varies greatly. The upper and front portions of the glenoid rim have a notch.[2]
This joint has a large range of motion at the expense of its stability due to the short, shallow glenoid cavity, the disproportionate size of the humerus head, and the loose articular capsule.[3] The body's shoulder joint dislocates the most commonly. The rotator cuff muscles' dynamic factors and the static Glenohumeral joint stability is influenced by factors related to the ligaments, labrum, and joint capsule. One of the risk factors for glenohumeral joint instability, which is one of the risk factors for rotator cuff disease, is the alignment of the humerus and the glenoid articular surfaces.[4], [5] For surgical treatments involving this bone, such as arthroscopic operations, metal fixation, drill hole placement, and prosthesis positioning, a thorough understanding of the glenoid cavity of the scapula is necessary.[6]
With this context in mind, the current study's goals were to collect morphometric data from the scapulae and the glenoid cavity, in particular the diameters and different glenoid shapes, for clinical use in joint replacement surgeries, the management of glenohumeral instability and rotator cuff tears, and to compare it to data from the local population.
Materials and Methods
Present study was approved by Institutional Ethical and Research committee [Registration No:PIMS/DR/RMC/2020/363] of a Pravara Institute of Medical Sciences, Loni. Adult human scapulae available from collection of dried bones in the department of Anatomy andfrom undergraduate students were used for study purpose.Scapulae of unknown age and sex were obtained
Inclusion criteria
Only fully ossified, dried, macerated and thoroughly cleaned scapulae which will be complete in all respects were included.
Exclusion criteria
The scapulae which were damaged and those having any deformity or pathology like healed fractures were excluded.
Sample size
After fulfilling inclusion and exclusion criteria 90 right and 90 left available Scapulae were selected for the study.
Vernier caliper
Following measurements metrical and non-metrical measurements were noted.
Metrical parameters
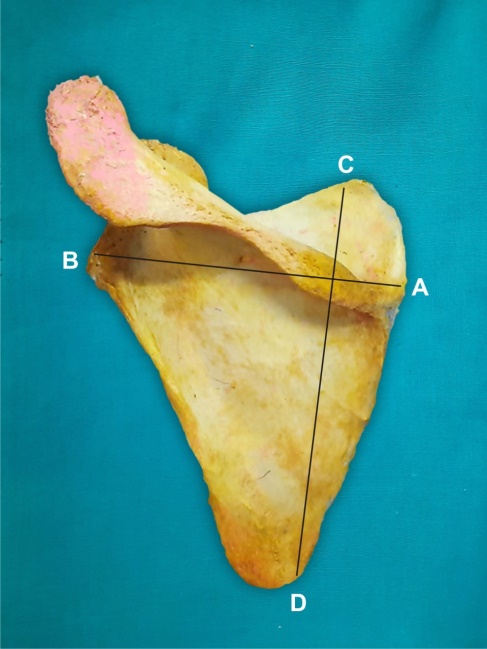
Maximum scapular length: It was measured from point ‘C’ at summit of superior angle to point ‘D’ at summit of inferior angle.([Figure 1])
Maximum scapular breadth: It was taken from point ‘A’ i.e. middle of the outer border of glenoid cavity to point ‘B’ where the spine intersects the vertebral border.([Figure 1])
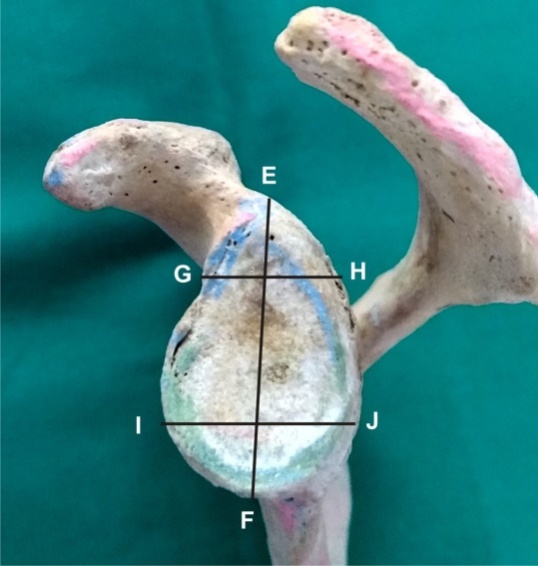
Height of glenoid cavity: it is maximum distance from inferior point on glenoid margin to the most prominent point of the supra-glenoid tubercle.([Figure 2])
Anteroposterior diameter 1: It is the maximum breadth of the articular margin of the glenoid cavity perpendicular to the glenoid cavity height.([Figure 2])
Anteroposterior diameter 2:It is the anteroposterior diameter (breadth) of the top half of the glenoid cavity.([Figure 2])
Nonmetrical parameter: Shape of glenoid cavity ([Figure 3], [Figure 4], [Figure 5])
Results
It is evident from [Table 1] length of scapula on right side was 135.40±13.2mm and on left side it was 136.5±12.9mm. Breadth of scapula on right side was 98.7 ±7.2mm on left side it was 98.2±6.8mm but the difference was not statistically significant. The height of Glenoid cavity on right side was 35.2±2.9mm and on left side it was 35.8±3.1. Antero-posterior diameter 1 of Glenoid cavity on right side was 24.2±2.3 mm and on left side it was 23.9±2.1 mm. Antero-posterior diameter 2 of Glenoid cavity on right side was 16.8±2.5 mm and on left side it was 16.7±2.4mm.
|
Type of measurements |
Side |
Sample size |
Mean±S.D |
T value |
P value |
|
Length of scapula |
Right |
90 |
135.40±13.2 |
0.56 |
0.5725 |
|
Left |
90 |
136.5 ±12.9 |
|||
|
Breadth of scapula |
Right |
90 |
98.7±7.2 |
0.47 |
0.6326 |
|
Left |
90 |
98.2±6.8 |
|||
|
Height of Glenoid cavity |
Right |
90 |
35.2±2.9 |
1.34 |
0.18 |
|
Left |
90 |
35.8±3.1 |
|||
|
Antero-posterior diameter 1 |
Right |
90 |
24.2±2.3 |
0.91 |
0.3621 |
|
Left |
90 |
23.9±2.1 |
|||
|
Antero-posterior diameter 2 |
Right |
90 |
16.8±2.5 |
0.27 |
0.78 |
|
Left |
90 |
16.7±2.4 |
|
S. No. |
Type of Shape |
Incidence of shape |
|
|
Right(n-90) |
Left(n-90) |
||
|
1 |
Pear |
46.66% (42) |
45.55%(41) |
|
2 |
Oval |
33.33% (30) |
40.00%(36) |
|
3 |
Inverted comma |
20.00% (18) |
14.44%(13) |
It is evident from [Table 2] that the most common shape of glenoid cavity was pear followed by oval and least common was inverted comma shape.



Discussion
The glenoid cavity was studied morphometrically using adult human scapulae. The measurements of the scapula and glenoid cavity in the present study were compared to those obtained by many authors, and several differences as well as commonalities were found. The length of the scapula in the current study was 135.40±13.2 mm on the right side and 136.5± 12.9 mm on the left side ([Table 1]). These results are in agreement with Dope et al. findings.’s that the average length of scapula was 136.74±14.13 mm on right side and134.29±15.54 0n left side among western Indian populations. Vardhan et al observation's of 137.94± 12.76 on the left side and 137.93± 12.88 on the right, which are close to our study.[7] The scapular length observed by Akhtar et al[8] was 135.70±14.3 on the right side and 134.9±14.1 on the left, which is close to the results of the current investigation. The length of the scapula measured by Rajeev Kumar et al[9] was 138.4 mm, which is consistent with our results.
The breadth of the scapula in the current study was 98.7±7.2 mm on the right side and 98.2±6.89 mm on the left side ([Table 1]). These findings are consistent with those of Dope et al.[10] who found that the right side's breadth was 97.97±9.07 mm and the left side's was 96.13±0.30 mm. Vardhan et al.[7] discovered that the scapular breadth was somewhat thicker on the right side (102.64±6.41) and the left side (102.76±7.16). It can be because of regional differences. Akhtar et al.[8] found that the right side scapular breadth was 97.97±9.07 and 97.02±0.30, which is consistent with our research. The breadth of the scapula measured by Rajeev Kumar et al[9] was 98.12 mm, which is consistent with our investigation.
In the current study, the glenoid cavity's height was 35.2±2.9 on the right side and 35.8±3.1 on the left ([Table 1]); in Dope et al.[10] study, the glenoid cavity's height was 37.03±3.55 on the right side and 36.52±4.12 on the left, which was closer to our study. Vardhan et al[7] measurment of the height of the glenoid cavity on the right side and left side, respectively, was 38.27±3.08 and 38.07±3.22, In a study by Akhtar et al.,[8] the glenoid cavity's observed height on the right side was 36.03±3.15 and on the left, it was 35.52±3.12. The height of the glenoid cavity in Rajeev Kumar et al[9] study was 36.4 mm, which is consistent with our investigation. Hetal et al.[11] measured the height of the glenoid cavity and found that it was close to our study on the right side (38.49±3.17 cm) and left side (38.06±3.34 cm). Gosavi et al[12] measurement of the glenoid cavity's height on the right side (35.03±5.25) and left (35.3±3.41) was comparable to what we found.
In the current study, the antero-posterior glenoid diameter 1 was 24.2±2.3 on the right side and 23.9± 2.1 on the left. ([Table 1]) When comparing with Dope et al.[10] the results on the right side were 24.61±3.53 and on the left, 24.56±4.47, which were closer to the results of our investigation. Antero-Posterior glenoid diameter 1 was found to be 24.04±2.67 on the right side and 22.85±2.44 on the left side by Vardhan et al.[7] which is consistent with our research. Antero-Posterior glenoid diameter 1 was 23.67±2.53 on the right side and 23.59±2.47 on the left, according to Akhtar et al.,[8] who made the observation. Antero-Posterior glenoid diameter 1 measured by Rajeev Kumar et al[9] was 25.36 mm, which agrees with the results of our investigation. Antero-Posterior glenoid diameter 1 on the right side was observed to be 24.76±2.49 and on the left to be 24.23±2.14, which was in close agreement with our study by Hetal et al[11] Antero-Posterior glenoid diameter 1 was discovered by Gosavi et al.[12] to be 24.17± 2.57 on the right side and 23.9± 2.66 on the left, which is comparable to our findings.
|
Studies |
Year |
Pear |
Oval |
Inverted comma |
||||
|
Right (%) |
Left (%) |
Right (%) |
Left (%) |
Right (%) |
Left (%) |
|||
|
Present study |
2022 |
46.66 |
45.55 |
33.33 |
40.00 |
20.00 |
14.44 |
|
|
Dope et al[10] |
2017 |
57 |
50 |
13 |
15 |
30 |
35 |
|
|
Vardhan et al[7] |
2019 |
47.28 |
54.92 |
30.90 |
32.40 |
21.82 |
12.68 |
|
|
Hetal et al[11] |
2018 |
44.44 |
47.37 |
38.89 |
34.21 |
16.67 |
18.42 |
|
|
Gosavi et al[12] |
2014 |
54.83 |
45 |
32.25 |
43.75 |
12.9 |
11.2 |
|
|
Arora et al[13] |
2019 |
38 |
71 |
35 |
15 |
27 |
13 |
|
|
Rajput et al[14] |
2012 |
49 |
46 |
16 |
15 |
35 |
39 |
|
|
Dhindsa et al[15] |
2014 |
48.78 |
46.15 |
21.95 |
17.94 |
29.26 |
35.89 |
|
|
Singh et al[16] |
2019 |
42.9 |
45.5 |
35.7 |
31.8 |
21.4 |
22.7 |
|
|
Akhtar et al[8] |
2016 |
51.59 |
49.02 |
13.49 |
13.73 |
34.92 |
37.25 |
|
Studies |
No of specimen |
Height of glenoid cavity |
Antero-Posterior glenoid diameter 1 |
Antero-Posterior glenoid diameter 2 |
|
Present study |
Right 90 |
35.2±2.9 |
24.2±2.3 |
16.8±2.5 |
|
Left 90 |
35.8±3.1 |
23.9±2.1 |
16.7±2.4 |
|
|
Dope et al[10] |
Right – 53 |
37.03±3.55 |
24.61±3.53 |
16.31±3.16 |
|
Left – 54 |
36.52±4.12 |
24.56±4.47 |
16.2.±3.64 |
|
|
Vardhan et al[7] |
Right 32 |
38.27 ± 3.08 |
24.04 ± 2.67 |
19.70 ± 2.23 |
|
Left 28 |
38.07 ± 3.22 |
22.85 ± 2.44 |
18.6 ± 2.07 |
|
|
Hetal et al[11] |
Right-36 |
38.49±3.17 |
24.76±2.49 |
18.83±2.19 |
|
Left-38 |
38.06±3.34 |
24.23±2.14 |
17.97±2.08 |
|
|
Gosavi et al[12] |
Right 62 |
35.03 ± 5.25 |
24.17± 2.57 |
14.56 ± 2.03 |
|
Left 80 |
35.3 ± 3.41 |
23.9 ± 2.66 |
14.6 ± 1.85 |
|
|
Arora et al[13] |
Right 48 |
34.44±2.07 |
22.99±2.77 |
17.48±1.82 |
|
Left 52 |
34.69±3.01 |
23.61±4.53 |
17.48±2.00 |
|
|
Rajput et al[14] |
Right 43 |
34.76±3 |
23.31±3 |
15.10±2.54 |
|
Left 57 |
34.43±3.21 |
22.92±2.80 |
13.83±2.45 |
|
|
Dhindsa et al[15] |
Right 41 |
34.13±3.16 |
24.05±2.86 |
|
|
Left39 |
34.11±2.57 |
23.36±2.22 |
|
|
|
Singh et al[16] |
Right 56 |
34.84±3.46 |
24.25±2.55 |
13.69±1.54 |
|
Left 44 |
33.48±2.88 |
25.52±2.78 |
12.01±1.77 |
|
|
Akhtar et al[8] |
Right 126 |
36.03±3.15 |
23.67±2.53 |
16.30±2.16 |
|
Left 102 |
35.52±3.12 |
23.59±2.47 |
16±2.34 |
In the current study, the antero-posterior glenoid diameter 2 was 16.8±2.5 on the right side and 16.7±2.4 on the left. ([Table 1]) When comparing with Dope et al.,[10] the results on the right side were 16.31±3.16 and on the left, 16.2±3.64, which were closer to the results of our investigation. Antero-Posterior glenoid diameter 2 was found by Vardhan et al.[7] to be 19.70±2.23 on the right side and 18.6±2.07 on the left, which is consistent with our research. Antero-Posterior glenoid diameter 2 was 16.30±2.16 on the right side and 16±2.34 on the left, according to Akhtar et al.,[8] who made the observation. Antero-Posterior glenoid diameter 2 measured by Rajeev Kumar et al[9] was 25.36 mm, which agrees with the results of our investigation. Antero-Posterior glenoid diameter 2 was 18.83±2.19 on the right side and 17.97±2.08 on the left, as observed by Antero-Posterior glenoid diameter 2 on the right side was 18.83±2.19 and on the left side was 17.97±2.08 according to Hetal et al[11] observations, which was in line with our investigation. Antero-Posterior glenoid diameter 2 was discovered by Gosavi et al.[12] to be 14.56± 2.03 on the right side and 14.6 ±1.85 on the left, which was comparable to our investigation.
The glenoid cavity's form in the current study was pear-shaped on the right side 46.66%, (42) while it was 45.55%(41) on the left. Next in the list were the shapes of an oval 33.33% (30) on the right side and 40% (36) on the left, and an inverted comma 20% (18) on the right side and 14.44% (13) on the left . Dope et al.[10] findings of pear-shaped 57% on the right and 50% on the left, oval-shaped 13% on the right and 15% on the left, and inverted comma-shaped 30% on the right and 35% on the left were higher than our estimate. Vardhan et al.[7] finding that the pear shape value is 47.28% on the right side and 54.92% on the left side is consistent with our research. Following the oval form which makes up 30.9% on the right side and 32.40% on the left are the inverted comma shape 21.85% on the right side and 12.68% on the left. However, inverted comma shape was the second most prevalent kind on the right side (34.92%) and on the left side (37.25%), while the oval type was the least prevalent on the right side (13.49%) and the left side (13.73%), according to Akhtar et al.[8] Hetal et al.[11] found that the pear shape was 44.44% on the right side and 47.37% on the left. Which was similar to our study, was followed by oval shapes on the right side (34.89%) and left (34.21%), which came in third place, and then an inverted comma 16.67% on the right side and 18.42% on the left. Gosavi et al.[12] discovered a pear-shaped glenoid cavity that was close to our study's findings on the right side (54.83%) and left (45%). Next least common kind is inverted comma shape on right side 12.9% and on left side 11.2%, followed by oval shape on right side 32.25% and on left side 43.75%.
Above all findings are compared with the previous studies in the [Table 3], [Table 4].
Conclusion
Knowledge of various measurements of Glenoid cavity is important for prosthesis of shoulder orthoplasty. It is useful in evaluation of various pathological conditions of shoulder joint. For orthopaedic surgeon size and shape of glenoid cavity is important. Since this study was conducted on limited number of scapulae further clinical, cadaveric and radiological studies are required.
Source of Funding
None.
Conflict of Interest
None.
References
- GS Dhindsa, Z Singh. A Study of Morphology of the Glenoid Cavity”. J Evol Med Dent Sci 2014. [Google Scholar]
- HB Rajput, KK Vyas, BD Shroff. A study of morphological patterns of glenoid cavity of scapula. 2012. [Google Scholar]
- MJ Akhtar, B Kumar, N Fatima, V Kumar. Morphometric analysis of glenoid cavity of dry scapulae and its role in shoulder prosthesis. Int J Res Med Sci 2016. [Google Scholar]
- A Singh, A Singh, P Agarwal. A Morphological and Morphometric Study of Glenoid Fossa of Scapula and its Implication in Shoulder Arthroplasty . Int J Anat Radiol Surg 2019. [Google Scholar]
- K Arora, NM Patel, BG Patel. Morphological study of glenoid cavity in dry human scapula. Int J Sci Res 2019. [Google Scholar]
- SN Gosavi, SD Jadhav, RS Garud. Morphometric study of scapular glenoid cavity in indian population. Int J Dent Med Sci 2014. [Google Scholar]
- H Vaishnani, K Jethva, A Rathwa, P Sharma. Morphometry and morphology of glenoid cavity of scapula. Int J Anat Res 2018. [Google Scholar]
- H Vardhan, M Chuhansk. Study of morphology of glenoid cavity of scapula; done on dry bone specimen in the department of anatomy of MGM medical college Jamshedpur. Int J Med Health Res 2019. [Google Scholar]
- SA Dope, D Dombed. Morphological and Morphometrical study of scapulae in Western Indian Population. Indian J Clin Anat Physiol 2017. [Google Scholar]
- D Johnson, P Girdle, S Standring, NR Borley, AR Crossman, MA Gatzoulis, JC Healy. Shoulder region and Axilla. Gray’s Anatomy, The Anatomical Basis of Clinical Practice 2013. [Google Scholar]
- AS Breathnach. . Frazer’s Anatomy of the Human Skeleton 1965. [Google Scholar]
- GJ Romanes. Upper and Lower Limbs. Cunningham‘s Manual of Practical Anatomy 1993. [Google Scholar]
- B J Brewer, R C Wubben, G Carrera. Excessive retroversion of the glenoid cavity, A cause of non-traumatic posterior instability of the shoulder. J Bone Joint Surg Am 1986. [Google Scholar]
- JQ Ly, DP Beall, TG Sanders. MR imaging of glenohumeral instability. AJR Am J Roentgenol 2003. [Google Scholar]
- S Rajan, S Ritika, K Js, SR Kumar, S Tripta. Role of coracoid morphometry in subcoracoid impingement syndrome. Int J Ortho Surg 2014. [Google Scholar]
- R Kumar. Assessment of variation of scapula- A Morphological study . HECS Int J Community Health MedRes 2017. [Google Scholar]