Introduction
The main function of lower limb in humans is to adapt itself for weight bearing and locomotion. The attainment of the erect posture has lead to the change in both the functional and mechanical requirements of skeletal elements of human body. Thus, there is a need for greater strength and stability in the lower limb compared to upper limb.1 Weight bearing is related to extended positions of the knee in case of humans. The knee joint is a complex synovial joint. A very important function of controlling the centre of body mass and posture is carried out by it. This needs a large range of movement in three dimensions coupled with the ability to withstand high forces. Many daily activities like walking, standing and climbing stairs are dependent on the knee joint. It is the main joint involved in jumping, running, kicking, etc. So, it is important to have an interaction between the articular surfaces, the passive stabilizers and the muscles that cross the joint, to maintain the range of mobility and stability.
The key component of knee joint is the proximal end of tibia which plays a very important role in transmission of body weight through tibio femoral articulation from the femur above and the talus below. Various forms of arthritis such as inflammatory and post traumatic arthritis affect the knee joint commonly. Among them, osteoarthritis is the most common pathology which is treated by total knee arthroplasty or unicompartmental arthroplasty. These arthroplasties require accurate soft tissue balancing and resection of bone thickness equal to the thickness of the prosthetic component implanted, so that the flexion-extension spacing are equal, allowing joint stability throughout the range of motion.
The different weight bearing situations and their relationships with antero-posterior and medio-lateral dimensions of diaphysis and epiphysis of tibia has been established well.2 There is a very important role of the knowledge of morphometry of upper end of tibia as it helps in providing the reliable method of assessment of deformities of knee. The morphometric parameters of upper end of tibia will help in guiding the treatment and further monitoring the outcome of total knee replacement surgeries. There is a need for an accurate and repeatable measurement system of the morphometric parameters of upper end of tibia because it will help the surgeon in defining the tibial deformity and hence tibial prosthesis design can be improved markedly.3 As surgeries of knee joint are rapidly evolving and technically demanding too, so a morphometric study of this region will definitely serve in the planning of various interventions needed in degenerative and other pathological conditions of knee.
Aims & Objectives
The present study was aimed to measure the different morphometric parameters of upper end of tibia and to establish its relation with total knee replacement.
Materials and Methods
The present study was a cross-sectional and prospective study. It was conducted on 50 adult tibia (25 of right side and 25 of left side) of unknown gender and age in the Department of Anatomy, Indira Gandhi Institute of Medical Sciences, Patna after obtaining the ethical clearance from the institutional ethics committee.
Inclusion criteria
Fully ossified, dried, macerated and thoroughly cleaned tibia which were complete in all respects in order to give correct observation.
Exclusion criteria
Tibia having any gross deformity or pathology.
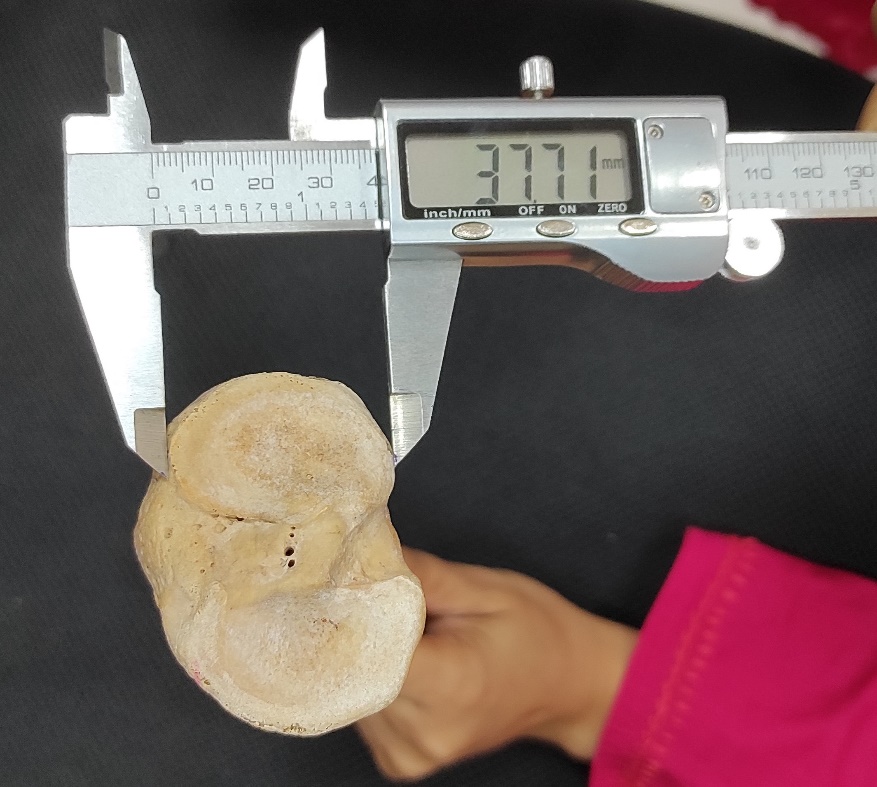
Different parameters were measured with the help of Vernier callipers with a least count of 0.01mm. The following morphometric parameters were noted (Figure 1)
Anteroposterior diameter of superior articular surface of medial condyle: The maximum distance between anterior and posterior borders of superior articular surface of medial condyle.
Transverse diameter of superior articular surface of medial condyle: The maximum transverse diameter of superior articular surface of medial condyle.
Anteroposterior diameter of superior articular surface of lateral condyle: The maximum distance between anterior and posterior borders of superior articular surface of lateral condyle.
Transverse diameter of superior articular surface of lateral condyle: The maximum transverse diameter of superior articular surface of lateral condyle.
Anteroposterior distance of intercondylar area: The maximum distance between anterior and posterior borders.
Transverse distance of intercondylar area: The maximum transverse diameter at following three levels: a) anterior end. b) middle narrow part (at the level of intercondylar eminence). c) posterior end.
The data thus obtained were tabulated and analysed statistically using Microsoft excel software.
Figure 1
Showing measurements of different parameters of upper end of left tibia;
ab & cd: Antero-posterior and transverse measurements of superior articular surface of lateral condyle.
ef & gh: Antero-posterior and transverse measurements of superior articular surface of medial condyle.
ij: Antero-posterior measurement of intercondylar area.
kl: Transverse measurement of intercondylar area at anterior end.
mn: Transverse measurement of intercondylar area at middle narrow part.
op: Transverse measurement of intercondylar area at posterior end

Results
The morphometric study on the adult tibia was performed and revealed the following results.
The mean values of antero-posterior diameters of medial condyle have been depicted in Table 1. It was found that the measurements were more on the right side, but the difference was statistically insignificant. The transverse diameter of medial condyle has also been depicted in Table 1. It was similarly found that they were more on the right side, but the difference was statistically insignificant. When the above two parameters were compared, it was found that antero-posterior diameter was more than transverse diameter in case of medial condyle on both the sides.
Table 1
Parameters of medial condyle
|
Diameters (mm) |
Right side Mean ± S.D. |
Left side Mean ± S.D. |
‘p’ value |
|
Antero-posterior |
47.90 ± 0.63 |
46.94 ± 0.46 |
0.483 |
|
Transverse |
30.08 ± 0.38 |
29.16 ± 0.43 |
1.07 |
The mean values of antero-posterior diameters of lateral condyle have been depicted in Table 2. It was found that the measurements were more on the right side, but the difference was statistically insignificant. The transverse diameter of lateral condyle has also been depicted in Table 2. It was found that they were more on the left side, but the difference was statistically insignificant. When the above two parameters were compared, it was found that antero-posterior diameter was more than transverse diameter in case of lateral condyle on both the sides.
Table 2
Parameters of lateral condyle
|
Diameters (mm) |
Right side Mean ± S.D. |
Left side Mean ± S.D. |
‘p’ value |
|
Antero-posterior |
40.62 ± 0.40 |
40.33 ± 0.17 |
0.587 |
|
Transverse |
28.54 ± 0.10 |
28.89 ± 0.05 |
0.993 |
When both the condyles were compared, it was found that both the antero-posterior and transverse diameters were more in case of medial condyle on both sides.
The antero-posterior diameter of inter-condylar area has been depicted in Table 3. It was found that the antero-posterior diameter was more on the left side, but the difference was statistically insignificant.
Table 3
Parameters of inter-condylar area
Transverse diameter of inter-condylar area was measured at 3 levels – anterior end, middle narrow part and posterior end. The values for the anterior end were more on the left side, but the difference was not significant statistically. Transverse diameter of middle narrow part was more on the left side and the transverse diameter of posterior end was more on the right side, but all the differences were insignificant statistically.
Table 4
Comparative table for the measurements of medial condyle
|
|
Antero-posterior diameter(mm) Mean ± S.D. |
Transverse Diameter(mm) Mean ± S.D. |
||
|
Right |
Left |
Right |
Left |
|
|
Present study |
47.90 ± 0.63 |
46.94 ± 0.46 |
30.08 ± 0.38 |
29.16 ± 0.43 |
|
Servien et al 4 |
50.8 ± 3.3 |
|
|
|
|
Gandhi S et al 5 |
48.45 ± 4.14 (male) 42.39 ± 4.19 (female) |
47.73 ± 4.37 (male) 42.36± 4.65 (female) |
30.18 ± 2.83 (male) 27.25 ± 3.05 (female) |
29.38 ± 3.14 (male) 26.96 ± 2.18 (female) |
|
P. Chaitanya et al 6 |
37.91 |
37.24 |
29.78 |
27.46 |
|
Ivan et al 7 |
40.8 ± 0.42 |
41.3 ± 0.42 |
|
|
|
Gupta et al 8 |
45.5 ± 0.29 |
43.6 ± 0.47 |
27 ± 0.24 |
27.6 ± 0.27 |
|
Bae & Park 9 |
48 ± 0.31 |
|
|
|
|
Srivastava et al 10 |
38.6 |
39.9 |
29.7 |
27.5 |
|
Ankur zalawadia et al 11 |
44.27 ± 1.93 (male) |
44.57 ± 2.18 (male) |
28.31 ± 1.66 (male) |
28.32 ± 1.35 (male) |
|
Muralimanju et al 12 |
40.60 ± 3.90 |
39.20 ± 3.60 |
26.90 ± 2.90 |
26.60 ± 2.70 |
|
Nayak G et al 13 |
41.7 ± 0.50 |
41.2 ± 0.42 |
27.8 ± 0.34 |
28.1 ± 0.59 |
|
Bhadoria P et al 14 |
45.36 ± 3.18 |
44.18 ± 4.25 |
29.86 ± 2.05 |
28.24 ± 2.89 |
|
Sinha B et al 15 |
43.4 ± 2.1 |
45.2 ± 2.6 |
28.5 ± 1.2 |
28.6 ± 1.4 |
|
Khurshid N et al 16 |
39.1 ± 0.39 |
26.1 ± 0.27 |
||
Table 5
Comparative table for the measurements of lateral condyle
|
|
Antero-posterior diameter (mm) Mean ± S.D. |
Transverse Diameter (mm) Mean ± S.D. |
||
|
Right |
Left |
Right |
Left |
|
|
Present study |
40.62 ± 0.40 |
40.33 ± 0.17 |
28.54 ± 0.10 |
28.89 ± 0.05 |
|
Servien et al 4 |
47.2 ± 3.3 |
|
|
|
|
Gandhi S et al 5 |
40.86 ± 3.79 (male) 36.78 ± 3.03 (female) |
40.69 ± 4.13 (male) 37.30 ± 3.81 (female) |
28.62 ± 3.10 (male) 26.14 ± 2.51 (female) |
28.82 ± 3.12 (male) 26.00 ± 3.06 (female) |
|
P. Chaitanya et al 6 |
36.89 |
37.42 |
29.37 |
29.95 |
|
Ivan et al 7 |
36.7 ± 0.41 |
35.4 ± 0.39 |
|
|
|
Gupta et al 8 |
40.8 ± 0.27 |
40.6 ± 0.40 |
26.6 ± 0.24 |
29.2 ± 0.32 |
|
Bae & Park 9 |
39.8 ± 0.29 |
|
|
|
|
Srivastava et al 10 |
36.4 |
36.9 |
29.2 |
29.7 |
|
Ankur zalawadia et al 11 |
38.26 ± 2.43 (male) |
38.51 ± 2.35 (male) |
27.13 ± 1.86 (male) |
27.38 ± 1.97 (male) |
|
Muralimanju et al 12 |
34.80 ± 3.90 |
32.60 ± 3.40 |
26.50 ± 3.40 |
25.70 ± 2.50 |
|
Nayak G et al 13 |
36.6 ± 0.31 |
39.2 ± 0.30 |
28.7 ± 0.55 |
31.2 ± 0.68 |
|
Bhadoria P et al 14 |
38.85 ± 2.75 |
39.26 ± 3.56 |
27.43 ± 2.08 |
28.08 ± 2.19 |
|
Sinha B et al 15 |
39.1 ± 2.5 |
38.9 ± 2.7 |
26.9 ± 1.5 |
27.6 ± 1.8 |
|
Khurshid N et al 16 |
35.1 ± 0.32 |
25.4± 0.31 |
||
Table 6
Comparative table for the measurements of antero-posterior diameter of Inter-condylar area
|
|
Antero-posterior diameter(mm) Mean ± S.D. |
|
|
Right |
Left |
|
|
Present study |
47.29 ± 0.06 |
49.06 ± 0.07 |
|
Gandhi S et al5 |
47.19 ± 2.93 (male) 43.09 ± 3.62 (female) |
49.11 ± 3.97 (male) 44.64 ± 3.94 (female) |
|
Kwak et al17 |
47.3 ± 3.8 |
|
|
Ivan et al7 |
42.5 ± 0.42 |
44.9 ± 0.44 |
|
Nayak G et al13 |
41.8 ± 0.44 |
43.1 ± 0.40 |
|
Khurshid N et al16 |
40.9 ± 0.44 |
|
Table 7
Comparative table for the measurements of transverse diameter of Inter-condylar area
|
|
Transverse Diameter(mm) Mean ± S.D. |
|||||
|
Anterior part |
Middle part |
Posterior part |
||||
|
Right |
Left |
Right |
Left |
Right |
Left |
|
|
Present study |
24.71 ± 0.55 |
26.13 ± 0.35 |
7.21 ± 0.26 |
7.85 ± 0.28 |
14.14 ± 0.44 |
13.24 ± 0.51 |
|
Gandhi S et al5 |
24.82 ± 3.22 (male) 22.33 ± 3.48 (female) |
25.40 ± 4.20 (male) 22.61± 2.41 (female) |
7.18 ± 1.14 (male) 6.72 ± 1.06 (female) |
7.41 ± 0.95 (male) 6.38 ± 0.79 (female) |
7.18 ± 1.14 (male) 6.72 ± 1.06 (female) |
7.41 ± 0.95 (male) 6.38 ± 0.79 (female) |
|
Jacobson et al18 |
35 Range (26-43) |
11 Range (7-14) |
16 Range (12-22) |
|||
|
Nayak G et al13 |
28.7 ± 0.55 |
31.2 ± 0.68 |
13.1 ± 0.20 |
12.5 ± 0.23 |
18.5 ± 0.42 |
12.8 ± 0.39 |
|
Bhadoria P et al14 |
26.76 ± 3.18 |
27.45 ± 4.18 |
9.25 ± 2.08 |
9.26 ± 1.05 |
11.24 ± 1.16 |
10.25 ±1.22 |
|
Khurshid N et al16 |
24.8 ± 0.37 |
13.6 ± 0.21 |
17.6 ± 0.27 |
|||
Discussion
Knee joint has a variable geometry and anatomy leading to difference in the morphometric parameters related to the upper end of tibia. This study attempted to find out the values of such parameters so as to provide a baseline data which will help in designing the various types of prostheses used in surgeries involving knee joint. The data obtained were found to be corroborative with some of the studies conducted earlier and different too from some other studies. It was found that the antero-posterior diameter was greater than the transverse diameter in case of both the condyles and medial condyle had greater diameters than the lateral condyle. Servian et al4 conducted their study on French population, independent of sex and side, and measured antero-posterior diameters of 19 medial and 18 lateral condyles. They found these to be 50.8+3.3mm and 47.2+3.3mm, respectively [Table 4, Table 5]. Their observation regarding medial condyle was close to the present study, but values of lateral condyle were not so close to the present study. Kwak et al17 also performed their study on 200 knees of 50 male and 50 female cadavers in Korean population. They measured antero-posterior diameter of intercondylar area which was very close to the present study [Table 6]. Jacobson et al18 studied transverse diameters of intercondylar area at 3 levels in Danish population by using 75 macerated dry specimens of human knee joint, but their findings were more than the present study at the first two levels and almost similar to the present study at the posterior most level [Table 7]. Swati Gandhi et al5 conducted their study on North Indian population on 50 male and 50 female tibia. Their values were very much corroborative with the present study [Table 4, Table 5, Table 6, Table 7]. Ivan et al7 conducted their study by dividing the bones into right and left sides and obtained almost similar results as that of the present study [Table 4, Table 5, Table 6]. Bae and Park et al9 measured the proximal tibia parameters for 173 knees and also obtained the similar values for the antero-posterior diameters of medial and lateral condyles as obtained in the present study [Table 4, Table 5]. Srivastava et al10 conducted their study in North Indian population on 150 dry tibia, 70 of right side and 80 of left side and found the values of different parameters lesser than the values obtained in the present study [Table 4, Table 5]. Gupta et al8 conducted their study in South Indian population by dividing the bones into 24 right and 26 left sides and obtained almost similar results as that of present study [Table 4, Table 5]. Bhadoria et al14 conducted their study in North Indian population by dividing the bones according to sex and side both (224 dry tibia of 112 males and females each, out of which 105 right and 119 of left side). The values of antero-posterior and transverse diameters of the two condyles were lesser than that obtained in the present study and the values for intercondylar area were almost similar to the present study [Table 4, Table 5, Table 7]. P. Chaitanya et al6 conducted a study on South Indian population on 50 dry tibia and obtained lower values for the medial condyle than the present study and almost similar values for the lateral condyle [Table 4, Table 5]. Zalawadia A et al11 conducted their study in Gujarat region on 120 tibia by dividing them into both sexes and two sides. They obtained lower values than the present study [Table 4, Table 5]. Nayak G et al13 conducted their study in Orissa on 46 tibia and obtained lower values than the present study [Table 4, Table 5, Table 6, Table 7]. Sinha B et al15 conducted their study on 50 tibia in Bihar population and obtained almost similar values as that of present study [Table 4, Table 5]. Khurshid N et al16 conducted their study on 30 tibia in Srinagar population and obtained lower values than the present study [Table 4, Table 5, Table 6, Table 7]. Muralimanju et al12 conducted their study on 73 tibia of South Indian population by dividing them into 2 sides and obtained lower values than the present study [Table 4, Table 5].
The various studies which have been performed in the past clearly indicate that there is a difference between the parameters of proximal end of tibia. This can be attributed to the racial variations of different populations. It has been previously seen that the bony features vary markedly among people of different ethnicities, so there is always a need to have data regarding such variations and studies conducted on different populations are very helpful in this regard.
Conclusion
The present study was undertaken to provide a baseline data of the various morphometric parameters of the upper end of tibia. It can now be concluded that this data will help in designing the different types of prosthesis being used in total knee arthroplasty and it will definitely help the orthopaedic surgeons in selecting the appropriate size of the prosthesis. It will also be helpful to the anthropologists and the forensic experts.