- Visibility 64 Views
- Downloads 13 Downloads
- DOI 10.18231/j.ijcap.2021.041
-
CrossMark

Magnetic resonance angiographic study of the variations in the branching pattern of external carotid artery
- Author Details:
-
 Rohita Salam *
Rohita Salam *
-
Sheela Sivan
Introduction
The common carotid artery, the external carotid artery and internal carotid artery are the major sources of blood supply to the head and neck. Clinical diagnosis and various surgical procedures in the head and neck region require a thorough knowledge of these arteries as well as their variations. A plethora of new and advanced surgical and imaging procedures in this area have made the study of these branching pattern and variations more relevant.
Conventionally the study of these variations has been studied in dissected cadaveric specimens. These have the disadvantages of failure to dissect out some branches like ascending pharyngeal artery, limited number of cadavers available for the study etc. Of late the use of magnetic resonance angiogram (MRA) of the head and neck region has opened a way to study the branching pattern of external carotid artery (ECA). This being a non-invasive, ionising radiation free method can help study the variations of branching of ECA. Studying the variations in a cadaver can be very well supported by MR angiographic study of the external carotid artery.
A thorough knowledge of subtle variations in the external carotid artery branching pattern may be helpful in the following circumstances:
In cases of severe epistaxis, ligation of external carotid artery or its branches may be done.
The external carotid artery is responsible for the major blood supply of head, neck and face and the knowledge regarding precise branching and supply pattern may be beneficial for plastic and reconstructive surgeons.
Arterial MR angiograms may be done pre operatively to map out the vascularity and the true extent of the tumours of the head, neck and face.
The vascularity of the tumours of head, neck and face may be decreased by selective arterial embolization.
Selective intra-arterial chemotherapy.
In carotid artery disease, a detailed knowledge of the branches of ECA arising from the ICA is important in diagnosing and treatment procedures.
Most major arteries in the body can be studied with the help of MRA. The carotid system in the neck and cerebral arterial system can be very well visualised by MRA. It can show the shape, size, location, orientation and variation, in these vessels. This information may be used for the better understanding of the branching pattern and variation of these arteries, which could be beneficial in the diagnosis and treatment of disorders related to these vessels.
Our aim is to study the anatomical variations and the branching pattern of external carotid artery in MR angiograms done for other purposes showing the carotid system.
Materials and Methods
The study was undertaken in our institution which is a tertiary care centre from the period September 2013 to September 2015. MR angiograms of patients attending the radiology department were used for studying the branching pattern and variations of external carotid artery.
MR angiograms of the carotid system taken for other purposes were used for our study. Only good quality images showing the branching pattern of external carotid arteries were included. Poor quality images and the ones not showing the relevant vessels were excluded.
Two independent observers studied the films and these variations were noted. The collected data was formulated and compared with previous studies.
Results
Of the 50 MR angiography studied, variations were seen in 5 cases.
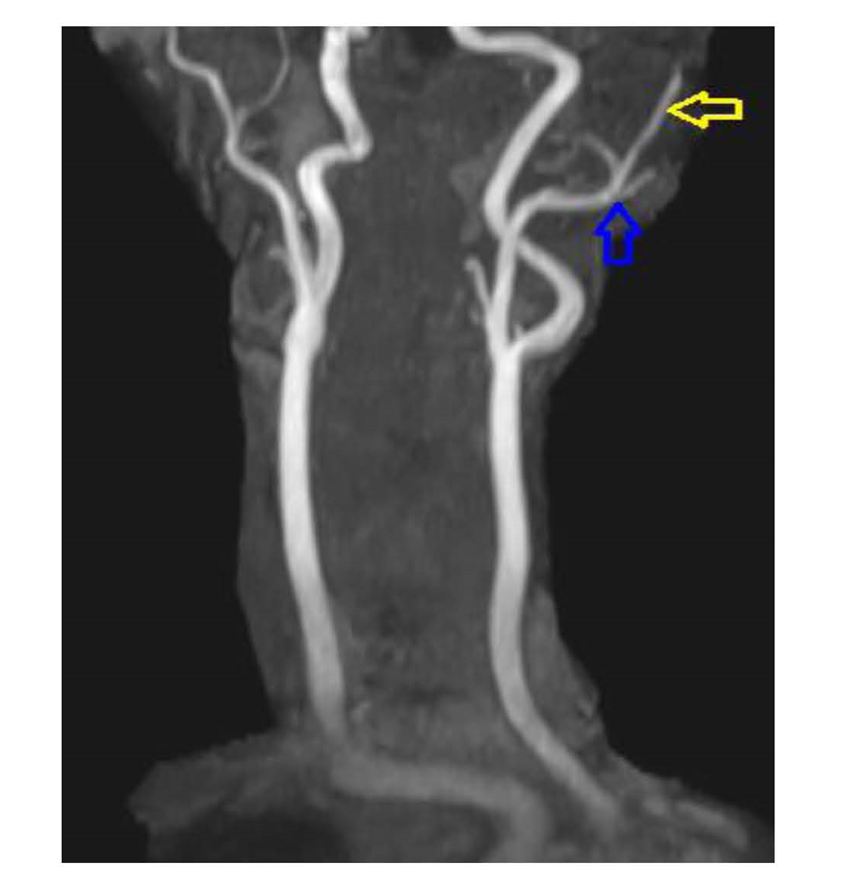
In two cases, the ascending pharyngeal artery arose from the lateral side instead of the medial side on the left side. ([Figure 1] )
In another two, the ascending pharyngeal artery arose from the occipital artery on the left side. ([Figure 2])
In one case, the superior laryngeal artery arose from the external carotid artery.
The incidence of variations in branching pattern of external carotid artery is 10% ([Figure 3]). There were no variations in the rest of the cases


Discussion
The external carotid artery begins lateral to the upper border of thyroid cartilage, between C3 and C4 vertebrae. It ascends forward and then passes backward little laterally and passes midway between the tip of the mastoid process and the angle of the mandible. In the stroma of the parotid gland behind the neck of the mandible, it divides into its two terminal branches the superficial temporal and maxillary arteries. From the origin of external carotid artery, as it ascends it gives off many branches which decreases in diameter.
The external carotid artery gives off eight branches distributed to the head and neck to supply the face and the neck region.[1], [2]
Superior thyroid artery
The first branch of the External carotid artery and it arises from the anterior surface of the ECA at a point just below the level of the greater horn of hyoid bone. It descends along the lateral border of the thyrohyoid membrane to reach the apex of the lobe of thyroid gland. It lies lateral to the inferior constrictor muscles and the external laryngeal nerve. The external laryngeal nerve is found often being posteromedial.
In approximately 16% of cases, the superior thyroid arises from the common carotid artery.
Ascending pharyngeal artery
It is the only branch arising from the medial side of ECA near the bifurcation of CCA. It ascends between the Internal carotid artery and the base of pharynx. It is crossed by the styloglossus and stylopharyngeus, and longus capitis lies posterior to it. It gives off branches to supply longus colli, sympathetic trunk, hypoglossal, glossopharyngeal and vagus nerves.
In approximately 14% of cases, the ascending pharyngeal artery arises from the occipital artery instead of arising from the ECA.
Lingual artery
It arises anteriorly and slightly medially from the ECA opposite the tip of the greater horn of hyoid bone between superior thyroid and facial arteries. Most often it arises from facial artery. Sometimes it arises from the superior thyroid artery. The lingual artery ascends vertically and reaches the inferior surface of the tongue as far as its tip.
Facial artery
The facial artery arises anteriorly from the ECA in the carotid triangle. It arises just above the lingual artery and immediately above the greater horn of the hyoid bone. It runs upwards and forwards, deep to the digastric and stylohyoid and winding around the submandibular and reaching the inferior surface of the mandible. The facial artery curves round inferior border of mandible anterior to the masseter and enter the face.
In most cases facial artery may arise in common with the lingual artery as a linguofacial trunk. Sometimes it may arise from the maxillary artery.
Occipital artery
It arises from the posterior surface of ECA. It is crossed superficially by the hypoglossal nerve at its origin and winds around it from behind. The artery then passes backwards, upwards and deep to the posterior belly of digastric. It then crosses the ICA, IJV, hypoglossal, vagus and accessory nerves. The occipital artery reaches the lateral border of rectus capitis lateralis between the transverse process of the atlas and the mastoid process.
In some cases, the occipital artery may arise from the ICA instead of ECA.
Posterior auricular artery
It arises from the posterior surface of ECA just above the origin of occipital artery. It ascends upwards and divides into auricular and occipital branches.
Posterior auricular artery may arise as a branch of occipital artery.
Superficial temporal and maxillary artery
These are the terminal branches of the ECA. Both the arteries arise within the stroma of the parotid gland. The superficial temporal artery continues the upward while the maxillary artery passes forward medial to the ramus of the mandible.
A rare case of combined high bifurcation of the common carotid artery, anomalous origin of the ascending pharyngeal artery and unusual branching pattern of the external carotid artery in dissected specimen was described by V Glunci et al.[3] The common carotid artery on the right side was found to bifurcate between the second and the third cervical vertebrae, giving rise to the ascending pharyngeal artery just below the bifurcation.
Jasmin Delik et al.[4] reported normal pattern of branching of ECA in 84% and branches arising from common trunks in 16%.
Uchino A and Saito N[5] found an anomalous artery arising from the proximal right external carotid artery on MR angiography.
Patil PV[6] and associates reported a case of anomalous origin of left vertebral artery from left carotid bulb during angiography.
Sirasapalli CN et al.[7] and associates reported a case of right ascending pharyngeal artery arising from the anteromedial wall of proximal right ICA, just 4 mm from its origin at the level of C3 vertebra in CT angiography.
Sirasapalli CN et al.[7] and associates reported an anomalous origin of right ascending pharyngeal artery arising from the anteromedial wall of proximal right internal carotid artery, just 4 mm from its origin at the level of C3 vertebra on CT angiography
[8]In the present study with the available MR angiograms, 45 cases showed normal branching pattern of external carotid artery. 4 cases showed variation in the origin of ascending pharyngeal artery. Usually in dissected specimen in cadaver, ascending pharyngeal artery is difficult to access. 1 case showed abnormal origin of superior laryngeal artery. Not many MR angiographic studies are available at present.
This study emphasizes on the need to have more MR angiographic studies of external carotid artery to have a better understanding about the variations of the branching pattern.
We had studied only 50 MR angiograms and that too from a single institution. This is a low number considering the possible variations in the branching pattern of ECA. This may be considered as a limitation of our study. So, a large multi centric study with a bigger number of MR angiograms may be done to get a better understanding on this.
Conclusion
MR angiogram of the carotid system is a good, inexpensive way to study the branching pattern of external carotid artery with no danger of ionising radiation.
Source of Funding
None.
Conflict of Interest
The authors declare no conflict of interest
References
- S Standring. . Gray’s Anatomy 2015. [Google Scholar]
- WH Hollinshead. . Anatomy for Surgeons 1968. [Google Scholar]
- V Gluncic, Z Petanjek, A Marusic, I Gluncic. High bifurcation of common carotid artery, anomalous origin of ascending pharyngeal artery and anomalous branching pattern of external carotid artery. Surg Radiol Anat 2001. [Google Scholar] [Crossref]
- J Delić, A Savković, A Bajtarević, E Isaković. Variations of ramification of external carotid artery - common trunks of collateral branches. Periodicum Biologorum 2010. [Google Scholar]
- A Uchino, N Saito. Persistent hypoglossal artery arising from the external carotid artery diagnosed by MR angiography. Surg Radiol Anat 2011. [Google Scholar] [Crossref]
- PV Patil, AM Patil, AV Apte, VY Attarde. Anomalous Origin of Left Vertebral Artery from Carotid Bulb Seen as "Trifurcation" of Left Common CarotidArtery with Acute Infarct in Ipsilateral Thalamus: A Case Report. J Neuroimaging 2015. [Google Scholar]
- CN Sirasapalli, T Mandapal, S Parida, M Belman. Anatomical Variant: Ascending Pharyngeal Artery Arising from the Extracranial Internal Carotid Artery. Indian J Vasc Endovasc Surg 2017. [Google Scholar]