- Visibility 139 Views
- Downloads 21 Downloads
- DOI 10.18231/j.ijcap.2020.064
-
CrossMark

A cadaveric study on variation in branching pattern of dorsalis pedis artery and its clinical perspectives
Introduction
Dorsalis pedis artery is the chief artery of the foot and is the continuation of the anterior tibial artery distal to the ankle. It passes to the proximal end of the first intermetatarsal space where it turns into the sole between the heads of the first dorsal interosseous to complete the plantar arch.[1]
Branches of dorsalis pedis artery
Lateral and medial tarsal arteries
Arcuate artery
First dorsal metatarsal artery
Cutaneous branches
The anatomical study of the arteries of the foot is necessary for further advances in arterial reconstruction. Such reconstruction often avoids amputation in cases of arterial trauma resulting from industrial and automobile accidents, as well as in patients with diabetes and severe ischemia of the lower limbs. The dorsalis pedis flap is one of the most common used foot flaps. There is still little detailed information on the arterial supply of the dorsum of the foot. Knowledge of the vascular anatomy is key to ensuring the safety and reliability of the flap surgery.
As variation in dorsalis pedis artery is uncommon, it is essential to have a sound knowledge about the artery it is advisable to have preoperative angiography for any abnormality, to prevent risks during surgical intervention. Hence the present work was undertaken to study in detail the abovementioned parameters and compare with the other workers.
Materials and Methods
44 lower limbs of unknown sex and age were obtained in a span of two years from the Department of Anatomy, Aarupadai veedu Medical College campus, Pondicherry, India The limbs were dissected carefully to explore the dorsalis pedis artery, and its branches was traced and painted and marked for clear view and photographed. They variations were observed were studied in details.
Observation and Results
Normal course and branches of dorsalis pedis artery
In the present study in 90% of cases the anterior tibial artery continued as the dorsalis pedis artery and gave the lateral tarsal artery, medial tarsal artery, arcuate artery and first dorsal metatarsal artery and continued as the deep plantar artery after piercing the first dorsal interoesseous muscle.
Dorsalis pedis artery was replaced by the peroneal artery
In specimens number 5RF and 5LF. The DPA was replaced by the peroneal artery and perforating branch which passes through the opening in the interoesseous membrane descended under cover of the extensor digitorum longus and peroneus tertius and anastomosed with anterior malleolar branch of anterior tibial artery.

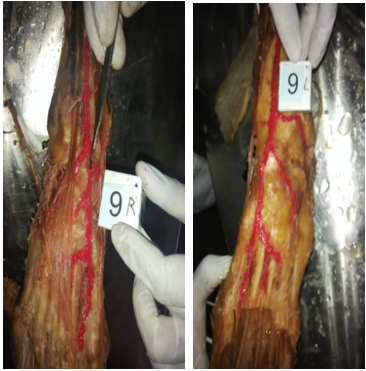
Anterior tibial artery was found on lateral side of leg
In specimen number 11RF and 11LF. Variation was observed, that is anterior tibial artery was found on lateral side of leg, dorsalis pedis artery is a continuation of the anterior tibial artery seen passing above lateral malleolus and then it passes forwards along the lateral side of the dorsum of the foot. It crossed inferior extensor retinaculum, below extensor digitorum longus and finally reached the proximal end of the intermetatarsal space.

Discussion
Variations in the blood vessel and their anomalous course can be attributed to their development. Tiny blood vessels derived from the blood islands in the 3rd or 4th week of development, merge with each other and form continuous network, from which buds grow out, canalize and form new vessels. New vessels of neighborhood areas form a closed network depending on the functional dominance, some vessels regress and others diverge in the mode of origin and course from the principal vessel. The dorsalis pedis artery is noted for its variations.[2]
The dorsalis pedis artery which is the continuation of anterior tibial artery is the main and prime arterial supply to the foot. It terminates at the proximal part of the first intermetatarsal space, where it divides into two branches, the first dorsal metatarsal artery and the deep planter artery and passes to it dips into the sole, between the head of first dorsal interoesseous muscle to complete the planter arch.[2] The present study was undertaken to study in details variation in the origin, course, and branching pattern of DPA in 44 specimens by dissection method.
Bailleul JP et al. reported that dorsalis pedis artery was replaced by perforating branch of peroneal artery in 8% of cases. Similar variation was observed in 12% of cases by Mestdagh H.B et al., in their study.[3] In the present study, the dorsalis pedis artery was replaced by perforating branch of peroneal artery in two specimen’s (5%) bilaterally.
Maral, tuncle M, Tas C reported that the posterior tibial artery traversing the interoesseous membrane, 5cm proximal to lateral malleolus and entered the extensor compartment, the anterior tibial artery failed to reach the ankle joint and was hypoplastic. In (8%) that is 4 out of 50 limbs the anterior tibial artery was hypoplastic and it is found that the dorsalis pedis artery was a continuation of peroneal artery, this variation was related tobacco smokers.[4]
Nilesh K. Mitra et al, reported in 14.29% of cases the second dorsal metatarsal artery originated from the dorsalis pedis artery which is not infrequent. In the present study, this variation was observed the second dorsal metatarsal artery originated normally from arcuate artery in all 44 specimens.[5]
Kesabi D, Keerti Singh et al., Lateral deviation of dorsalis pedis artery and higher bifurcation of anterior artery tibial artery to form dorsalis pedis at junction of upper 3/4th and lower 1/4th of leg. In the present study found that dorsalis pedis artery begins in front of the ankle between the two malleoli was in all specimens, expect 10% of specimen.[6]
The significance of the above discussed variation of the dorsalis pedis artery are extremely important for cardiologists, Interventional Radiologists, Plastic Surgeons, Traumatological surgeons these days. This artery is used to record peripheral arterial pulsation. Also the musculo-cataneous flaps based on dorsalis pedis artery are commonly used for reconstructive surgeries.
The present work was undertaken to study the variations of the dorsalis pedis artery regarding origin, variation, branching pattern. Because dorsalis pedis artery and surrounding flap have great clinical applications. Very frequently they are approached and, used by cardiologists, Interventional Radiologists, Plastic Surgeons, and Traumatological Surgeons.
Conclusion
In the present work, recording the dorsalis pedis artery variation, out of 44 specimens, 40 were normal in their origin, course, branching pattern and termination.
In 5% the dorsalis pedis artery was replaced by perforating branch of the peroneal artery. The perforating branch which passes through the opening in the interoesseous membrane and descended under cover of extensor digitorum longus and peroneus tertius and anastomosed with the anterior malleolar branch of anterior tibial artery.
In 5% the anterior tibial artery runs along lateral side of the leg and continues as dorsalis pedis artery passes above lateral malleolus, and then passes forward along the lateral side of the dorsum of the foot.
The knowledge of dorsalis pedis artery origin, variations, branching pattern are indispensable for clinicians. Dorsalis pedis artery and fascio-cutaneous dorsum of foot flap are used as graft. Dorsalis pedis arteries are approached by cardiac Surgeons, Interventional Radiologists, Plastic Surgeons and Traumatological Surgeons. Hence the present work has great relevance clinically.
Source of Funding
None.
Conflict of Interest
None
References
- T Sadler. . Lang man’s Medical Embryology 1985. [Google Scholar]
- Y Mamatha, . R Sunitha, Om K V Prakash. Variation in Branching pattern of Dorsalis pedis Artery: A case report. Int J Recent Sci Res . [Google Scholar]
- J P Bailleul, P R Olivez, H Mestdagh, B Vilette, R Depreux. Descriptive and topographical anatomy of the dorsal artery of the foot. Bull Assoc Anat (Nancy) 1984. [Google Scholar]
- T M Maral, T C Celik. Anomalous dorsalis pedis artery. Surg Radial Anta 1994. [Google Scholar]
- N K Mitra, O A Habbal, A H El-Hag, N A Al-Hashmi. Bilateral absence of the Arcuate artery on the Dorsum of the Foot. Sultan Qaboos Univ Med J 2007. [Google Scholar]
- D Kesavi, K Singh, M S Rajendran. Analogous course of Dorsalis pedis artery. Anat Adjuncts 2002. [Google Scholar]