- Visibility 92 Views
- Downloads 21 Downloads
- DOI 10.18231/j.ijcap.2020.060
-
CrossMark

A cadaveric study of morphology and morphometry of petrous and cavernous parts of the internal carotid artery
Introduction
Internal carotid artery [ICA] arises from the common carotid artery at the level of the upper border of the thyroid cartilage. Its course is divided into four parts, namely the cervical, petrous, cavernous and cerebral parts. Cervical part has a vertical extent from its origin to the base of the skull. It then enters the lower end of the carotid canal that lies within the petrous temporal bone. The petrous part runs through the carotid canal and traverses the foramen lacerum, before entering the cavernous sinus. The cavernous part runs forwards within the sinus from behind forwards and exits the sinus by piercing its dural roof at the anterior end. Now it is seen in relation to the base of the brain and is called the cerebral part. The branches arising from the petrous part are the carotico-tympanic and pterygoid arteries, and those from the cavernous part are the cavernous, hypophyseal and meningeal branches.[1]
Petrous part of the artery follows the curvatures of the carotid canal. Cavernous part has a slightly tortuous appearance generally, but when it is marked, it has been described as redundant curvature.[2] Variations in the length and calibre of the vessel have been reported to affect the haemodynamics of the vessel. Understanding this altered hemodynamics is essential in managing patients with vascular conditions like cerebrovascular accidents.[3]
Aneurysm affecting the petrous and cavernous parts of the ICA have been described in literature. They are generally reported to be idiopathic and do not cause any symptoms. They are generally noticed incidentally during radiological studies.[4] Aberrant course of the petrous part of ICA with bony dehiscence of the carotid canal into the middle ear cavity, resembling a retro-tympanic mass, and as a cause of hearing loss, has also been reported in literature.[5]
Awareness of variations in the course and dimensions of the petrous and cavernous parts of the ICA would be useful for radiologists in interpreting the findings on cranial contrast arteriography, MR angiography and duplex ultrasonography. Otolaryngologists and neurosurgeons contemplating head and neck surgeries and skull base surgeries should be aware of the variations affecting these segments of the arteries in order to prevent complications.
In view of the paucity of literature on these two parts of the artery, the present study was conducted to evaluate the variations in the morphology of the petrous and cavernous parts of the ICA, along with the morphometric analysis.
Materials and Methods
The study was carried out on both sides of 25 head and neck specimens obtained from human cadavers of both the sexes, that were routinely used for undergraduate teaching. It was conducted in the Department of Anatomy, Pushpagiri Institute of Medical Sciences and Research Centre, Thiruvalla. Specimens that showed gross deformities were excluded from the study. The ICA was dissected using the Cunningham method.
Following removal of the brain, sagittal sections of the head and neck specimens were taken. The petrous part was exposed by breaking open a part of the petrous temporal bone (using a chisel and mallet), bordered by the internal acoustic meatus, superior petrosal sinus and the foramen lacerum. The cavernous part was exposed by opening the roof of the cavernous sinus. The curvatures of the two parts of the arteries were studied and variations in their curvatures were noted down.
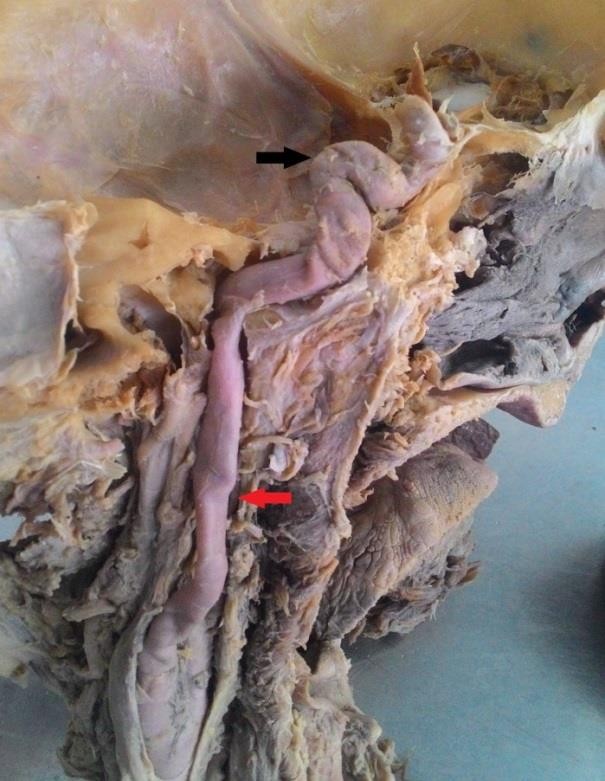
The length of the petrous part was measured from the lower end of the carotid canal to its upper end. ([Figure 1]) The thread was carefully traced along the curvature of the vessel within the canal. The length of the cavernous part was measured from its point of entry within the cavernous sinus to its exit from it by piercing its dural roof ([Figure 2]) The length of both parts was measured using a thread and ruler.
The diameter of the petrous part was measured at the lower end of the carotid canal, and that of the cavernous part was measured at the posterior end of the sinus, using a Vernier caliper. The morphological parameters were expressed in cms. Their mean and standard deviation were calculated and analyzed using paired t test. And a p-value less than 0.05 was considered to be significant.
Results
Out of the 50 specimens, 25 belonged to the right side and 25 belonged to the left side. Differentiation of the sex of the specimens was not done.
Petrous part of ICA showed consistent pattern of curvature within the carotid canal in all the specimens. Redundant curvature of the cavernous part of the artery was observed in 15 specimens (30%), one of them had aneurysm associated with it ([Figure 3]). Redundant curvature was noted with greater frequency on the right side. These specimens showed significantly greater length and the diameter compared to those without redundant curvature (p<0.05).
In one specimen, on the right side (2%) aneurysm was seen in both petrous and cavernous parts. In yet another specimen, again on the right side (2%), it was noted in petrous part only. And in total 5 specimens (10%) – 3 left-sided and two right-sided; aneurysm was noted in cavernous part only. Statistically significant increase in the diameter was noticed in those specimens with aneurysm in both the petrous (p<0.001) and cavernous parts (p=0.000).
The mean length and diameter of the petrous and cavernous parts of the ICA are given in [Table 1].
| Mean length (cm) | Mean diameter (cm) | |||||
| Right (n=25) | Left (n=25) | Total (n=50) | Right (n=25) | Left (n=25) | Total (n=50) | |
| Petrous part | 3.83 ± 0.45 | 3.88 ± 0.33 | 3.8 ± 0.39 | 0.52 ±0.33 | 0.46 ± 0.08 cm | 0.49 ± 0.24 |
| Cavernous part | 3.62 ± 0.45 | 3.57 ± 0.47 | 3.59 ± 0.46 | 0.48 ± 0.11 | 0.48 ± 0.1 | 0.48± 0.1 |


Discussion
As per review of literature, ICA within the carotid canal, initially runs upwards and laterally and then turns medially, making an acute curvature. As the artery reaches the foramen lacerum, it gradually bends forwards making an obtuse angle. It runs over the cartilage covering the foramen lacerum to reach the posterior end of the cavernous sinus. Our present study showed consistent course and curvatures of the petrous part of the ICA in all the specimens. The curvatures of the petrous part of the ICA was studied in detail by Vijaywargiya et al. in 2017.[6] They reported the angle of the first bend to be ranging from very acute to obtuse. But they found less variability in the angulation of the second curvature.
The cavernous part of the ICA is generally described to have a small amount of tortuosity. In our study, redundant curvature as marked by pronounced tortuosity was noticed in eight right sided and seven left sided specimens. The total frequency obtained (30%) is comparable to that (33%) observed by Jittapiromsak P et al. in their study on nine cadaveric head and neck specimens.[2]
The intra-cavernous curve of the ICA correlates with the curvature of the skull. The intra-cavernous arterial branches and intra-cavernous neural structures lie close to each other in normal type of curvature. But they lie away from each other in the redundant type. Thus there could be an intraoperative risk of neural compression in this region in patients with normal curvature.[2]
Aneurysms affecting the petrous part of the artery have been described earlier in the literature. Most of them being case reports, there is little data available on the frequency of aneurysm involving the petrous part. They are usually congenital and discovered accidentally in patients while doing CT scans for other reasons.7We noticed aneurysm in the petrous part in only 2 specimens (4%), and both were right sided.
| Vijaywargiya et al. 20176 [cadaveric study] (n= 56) | Takegoshi H et al. 20077 [radiological study] (n=345) | Isik Tuncer 2018 8 [radiological study] (n=49) | Present study (cadaveric study) (n=50) | ||
| Petrous part | Length (cm) | 3.1 | 2.67 | Not studied | 3.8 ± 0.39 |
| Diameter (cm) | 0.4 | 0.57 | Not studied | 0.49 ± 0.24 | |
| Cavernous part | Length (cm) | 3.79 | Not studied | Not studied | 3.59 ± 0.46 |
| Diameter (cm) | 0.39 | Not studied | 0.5±0.6 | 0.48± 0.1 |
Sometimes, these aneurysms are large at the time of diagnosis and are often associated with large thrombus.[9], [10] They are reported to be the cause of varied symptoms like headache, nasal congestion, hearing loss and tinnitus in those patients. Further, rupture of the aneurysm as an initial manifestation of the aneurysm has been reported in approximately 25% of cases.[11] Giant aneurysm in the petrous part with a thrombus clinically presenting as stroke,[11] and pseudo- aneurysms, secondary to infections in adjoining areas were also reported.[12], [13]
Aneurysm of cavernous part of ICA was reported by several authors.[14], [15], [16] In the present study, we noticed intra-cavernous aneurysm in 3 left sided and 2 right sided specimens (10%). In one specimen on the right side, the aneurysm coexisted with redundant curvature.
Aneurysms in the cavernous part of ICA tend to grow from large to giant size before they manifest clinically. Giant aneurysms causing compression of adjacent structures and presenting with features of paralysis of adjacent cranial nerves have been described earlier. Rupture of these aneurysms is rare and results in direct communication between the carotid artery and cavernous sinus.[4]
Review of literature shows only one cadaveric study by Vijaywargiya et al. (2017) on the length and diameter of petrous and cavernous parts of the artery.[6] The length and diameter of the petrous part of the artery were measured on CT scan by Takegoshi et al. in 2007[7] and diameter alone of the cavernous part by Isik Tuncer in 2018.[8] The findings of our study in comparison with their findings are given in [Table 2].
The values obtained in our study were slightly on the higher side than those obtained by Vijaywargiya et al.[6] except for the length of the cavernous part, which was almost similar. The mean diameter obtained in our study was slightly lesser than those obtained in both the radiological studies. Whereas the length of the petrous part was higher than that obtained on the radiological study by Takegoshi et al.[7]
In specimens having redundant curvature of the cavernous part of the artery, a statistically significant increase in length and diameter of the artery was observed. Similar observations were noticed by Vijaywargiya et al.[6] They also observed that increasing length resulted in sharper angulations. These findings strongly suggest that longer and tortuous arteries indicate underlying increased hemodynamic stress. Specimens showing aneurysm showed significant increase in the diameter of the vessel in both petrous and cavernous parts, whereas the length of the same showed significant increase in the petrous part only.
Sometimes, the petrous part of the artery can have an aberrant course, causing dehiscence of the bony carotid canal, giving the appearance of a non-pulsatile mass in the tympanic cavity. This imposes diagnostic challenges to the otolaryngologists.[5] But we did not come across any such aberrant course of the vessel. Congenital unilateral absence of the ICA with inter-cavernous anastomosis was also reported earlier.[17], [18]
Thorough knowledge of the variations in the course, curvatures and morphometrical parameters of the petrous and cavernous parts of the ICA will give a diagnostic edge to the radiologists. It is also essential to the otolaryngologists and neurosurgeons contemplating to perform procedures like endoscopic skull base surgeries. This would help to avoid devastating consequences that can occur when the vessel is inadvertently injured in surgical exploration.
Conclusion
Petrous part of the ICA is generally constant in its course and curvatures within the carotid canal, whereas redundant curvature is present in approximately 30% of the arteries in their cavernous parts. Redundant curvature of the cavernous part always presents with increase in length and diameter of the artery. Aneurysms are present in the petrous and cavernous parts with a frequency of 4% and 10% respectively. They are associated with significant increase in the diameter of the vessel. The mean length and diameter of the petrous and cavernous parts ranges from 3.5 – 4 cm and 0.5cm respectively.
Abbreviations
ICA - Internal carotid artery, MR - Magnetic resonance
Conflicts of Interest
None
Source of Funding
None
References
- S Standring, A R Crossman. Neuroanatomy: Vascular supply and drainage of the brain. Gray’s Anatomy 2008. [Google Scholar]
- P Jittapiromsak, H Sabuncuoglu, P Deshmukh, C McDougall, R Spetzler, M Preul. Anatomical Relationships of Intracavernous Internal Carotid Artery to Intracavernous Neural Structures. Skull Base 2010. [Google Scholar]
- S Kamath. Observations on the length and diameter of vessels forming the circle of Willis. J Anat 1981. [Google Scholar]
- B G Welch, H H Batjer. Cavernous Carotid Aneurysms: You Can But Should You?. World Neurosurg 2014. [Google Scholar]
- T Muderris, S Bercin, E Sevil, H Cetin, M Kiris. A Potentially Catastrophic Anatomical Variation: Aberrant Internal Carotid Artery in the Middle Ear Cavity. Case Rep Otolaryngol 2013. [Google Scholar]
- M Vijaywargiya, R Deopujari, S A Athavale. Anatomical study of petrous and cavernous parts of internal carotid artery. Anat Cell Biol 2017. [Google Scholar]
- H Takegoshi, S Kikuchi. An anatomic study of the horizontal petrous internal carotid artery: Sex and age differences. Auris Nasus Larynx 2007. [Google Scholar]
- I Tuncer. Angiographic morphometry of internal carotid, external carotid and common carotid artery in Turkish adult. Int J Med Health Res 2018. [Google Scholar]
- J T Patrick. Magnetic Resonance Imaging of Petrous Carotid Aneurysms. J Neuroimag 1996. [Google Scholar]
- R W Urwin, R T Higashida, V V Halbach. Endovascular therapy for the carotid artery. Neuroimag Clin N Am 1996. [Google Scholar]
- V Akgun, S Sari, S Verim, U Bozlar. Giant petrosal aneurysm of the internal carotid artery causing stroke in a young man. Case Rep 2013. [Google Scholar] [Crossref]
- H Tanaka, U Patel, D A Shrier, J U Coniglio. Pseudoaneurysm of the petrous internal carotid artery after skull base infection and prevertebral abscess drainage. AJNR Am J Neuroradiol 1998. [Google Scholar]
- C J Hwang, G Moonis, R W Hurst, N Hockstein, D Bigelow. Bilateral petrous internal carotid artery pseudoaneurysms presenting with sensorineural hearing loss. AJNR Am J Neuroradiol 2003. [Google Scholar]
- I Wanke. Carotid cavernous fistula due to a ruptured intracavernous aneurysm of the internal carotid artery: treatment with selective endovascular occlusion of the aneurysm. J Neurol, Neurosurg Psychiatry 2001. [Google Scholar]
- F Akai, S Nakagawa, T Fukawa, H Yugami, M Taneda. Symptomatic Cavernous Internal Carotid Artery Aneurysms Treated with Detachable Coils. Interv Neuroradiol 2003. [Google Scholar]
- T Ohmoto, S Nagao, S Mino, T Ito, Y Honma, T Fujiwara. Exposure of the Intracavernous Carotid Artery in Aneurysm Surgery. Neurosurg 1991. [Google Scholar]
- R B Midkiff, M W Boykin, D R Mcfarland, J A Bauman. Agenesis of the internal carotid artery with intercavernous anastomosis. AJNR Am J Neuroradiol 1995. [Google Scholar]
- A Kumaresh, P K Vasanthraj, A Chandrasekharan. Unilateral Agenesis of Internal Carotid Artery with Intercavernous Anastomosis: A Rare Case Report. J Clin Imaging Sci 2015. [Google Scholar]