Introduction
Internal carotid artery (ICA), the major paired artery to the brain, arises from the common carotid artery at its bifurcation. Its origin corresponds to the upper border of thyroid cartilage, at a level between the third and fourth cervical vertebrae. It has got four parts, namely cervical, petrous, cavernous and cerebral. The cervical part begins from its origin to the base of the skull. It ascends to enter the carotid canal in the petrous temporal bone. No branches are given off from this part.1 Knowledge of variations in the origin and course of ICA would be useful for radiologists in interpreting cranial contrast arteriography, MR angiography and duplex ultrasonography, and for surgeons while performing various head and neck surgeries and stenting procedures.
Materials and Methods
Fifty formalin fixed head and neck specimens were obtained from adult cadavers of both sexes in the dissection hall of Department of Anatomy at Pushpagiri institute of medical sciences and research centre, Tiruvalla. Specimens with gross deformities were excluded from the study. By cadaveric dissection, the ICA was studied noting down the variations in its origin and course of the cervical part of the vessel. The cervical part was approached through dissection of the carotid triangle. The carotid triangle was defined by its boundaries and the carotid sheath was traced from the root of the neck to the skull base. The contents of the triangle were exposed by opening up the sheath. The ICA was traced from its origin at the carotid bifurcation to its entry into the base of the skull. The level of origin was noted with reference to the upper border of thyroid cartilage. Variations at the level of origin and morphology of cervical part of ICA were noted and photographed.
Results
Out of the 50 specimens, 25 belonged to the right side and 25 belonged to the left side. Differentiation of the sex of the cadavers was not done.
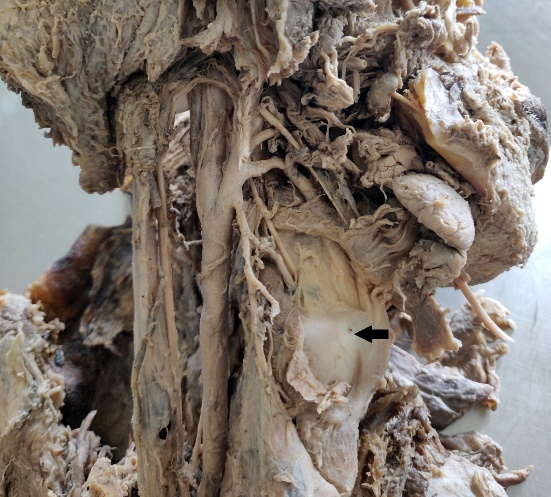
Among the specimens studied, 30 specimens (60%) showed normal origin and 20 specimens (40%) had variations in their origin. Among those specimens with variations, 19 specimens (38%) had high origin (Figure 1) and one specimen (2%) had low origin of the artery. High origin of ICA was found on the right side in ten specimens (40%) and on the left side in nine specimens (36%). Low origin was found only in one specimen on the right side (4%). (Table 1)
Table 1
Incidence of variations in the origin with side
| Origin | Side | Total | ||||
| Right | Left | |||||
| No. | % | No. | % | No. | % | |
| Normal | 14 | 56.0 | 16 | 64.0 | 30 | 60.0 |
| High | 10 | 40.0 | 9 | 36.0 | 19 | 38.0 |
| Low | 1 | 4.0 | 0 | 0.0 | 1 | 2.0 |
| Total | 25 | 100.0 | 25 | 100.0 | 50 | 100.0 |
The cervical part of the ICA was found to be normal in 17 specimens (34%) and showed variations in 33 specimens (66%). (Table 2)
Table 2
Variations in the cervical part
| Cervical part | Frequency | Percentage |
| Normal | 17 | 34 |
| Variant | 33 | 66 |
| Total | 50 | 100 |
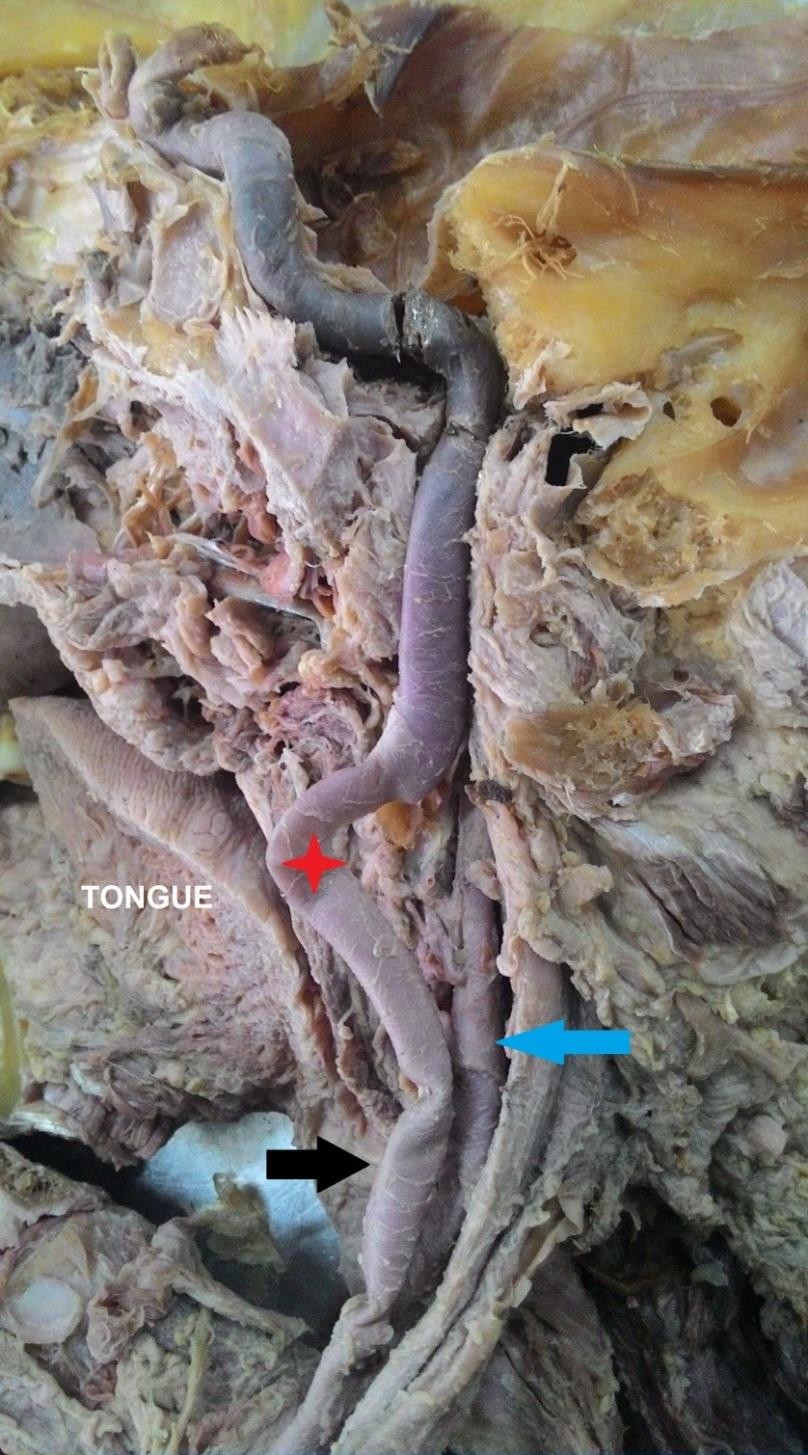
Majority of the variations observed were kinks (Figure 2), seen in 16 specimens (32%) followed by curving (Figure 3) of the ICA in 9 specimens (18%). Other variations noted were tortuosity of the vessel in 5 specimens (10%), coiling (Figure 4) and loop formation in 3 specimens (6%), and aneurysm formation and aberrant course (Figure 5) in 2 specimens each (each contributing to 4%).
Out of the 16 specimens showing kinks, 6 were noted on the right side and 10 were on the left side. Similarly, 9 specimens with curving of the ICA were found to be distributed as 4 on the right side and 5 on the left side. Out of the 5 specimens with tortuosity, 3 were on the right side and 2 were on the left. Two specimens on the right and 1 specimen on the left showed coiling and loop formation of the ICA. The incidence of aneurysm formation seemed equal on the two sides, with one on either side. The aberrant course of the ICA was noted on the right side in 2 specimens. (Table 3)
Table 3
Incidence of variations in the cervical part with side
| Variations | Side | Total | ||||
| Right | Left | |||||
| No. | % | No. | % | No. | % | |
| Kink | 6 | 24 | 10 | 40 | 16 | 62 |
| Curve | 4 | 16 | 5 | 20 | 9 | 18 |
| Tortuosity | 3 | 12 | 2 | 8 | 5 | 10 |
| Coiling | 2 | 8 | 1 | 4 | 3 | 6 |
| Aneurysm | 1 | 4 | 1 | 4 | 2 | 4 |
| Aberrant | 2 | 8 | 0 | 0 | 2 | 4 |
Two specimens with aberrant course of the ICA on the right side were found to have kinks. Significant correlation between the aberrant course of the ICA and the occurrence of the kinks was observed on the right side. There were 2 cases with coiling showing aneurysms.



Discussion
The normal pattern of origin of the ICA from the Common carotid artery, at its bifurcation at the level of the upper border of the thyroid cartilage, was seen only in 60% of the study specimens.
High origin of the ICA, arising above the level of the upper border of thyroid cartilage was found in 40% of the specimens on the right side and 36% on the left side. This is slightly closer to frequency of higher origin (46.65%) reported by Al-Rafiah A et al. in 2011.2 But the frequency of high origin in the present study is much lower than the findings of the previous studies. High origin of ICA was reported to be 64% on the left and 50% on the right by Anu VR et al. in 2007,3 and 60% on the left side and 55% on the right side by Zumre O et al. in 2005.4 In both the studies, higher origin was more frequent on the left side in contrast to this study.
Lower level of origin of the vessel was seen in only one case in this study, which was on the right side (2%). Literature review also shows less frequency of lower origin of ICA. It varied from 1%-10% in various studies.2, 3, 4
Normal cervical part of the vessel was found in 34% of the specimens. Variations were noted in 66% of the specimens and were of kinks in 16 specimens (32%), curvatures in 9 specimens (18%), tortuosity in 5 (10%), coiling/ looping in 3 (6%), aberrant course in 2 (4%) and aneurysm in 2 specimens (4%).
Majority of the variations in the present study were kinks followed by curves and tortuosity. Most of the variations were found to be on the left side in this study. A similar study was conducted by Friedrich Paulsen et al. in 2000. They analyzed 282 specimens and summarized that 191 specimens (68%) had straight course, 74 specimens (26%) had curved course, 12 showed kinking (4.2%) and 5 showed coiling (1.7%). They also reported that there were no side and sex differences among the variations.5
Tortuosity was observed in only 5 specimens (10%) in this study. Tortuosity of ICA was observed in detail by John Cairney in 1924 and reported 16.67% of tortuosity in his study sample.6
The frequency of aberrant course of the vessel in the present study is much higher than that reported (0.2%) by Munoz A et al. in 2010.7 In the present study, 2 specimens (4%) were found to be arising medial to the ECA close to the hypopharynx. Kinking of the vessel was also noted in both the cases of aberrant course.
Aneurysm was observed in only 2 cases (4%) in the present study, associated with coiling in both of them. Aneurysm of cervical part of ICA was first described by Sir Astley Cooper in 1808.8
Curved course, tortuosity, kinking and coiling are considered to be congenital anomalies. These can be explained on the basis of the embryological development. The ICA develops from the 3rd aortic arch and from the dorsal aorta. Initially at the junction between these 2 blood vessels, a loop is present normally. Later on with the descent of the heart and the large vessels into the mediastinum, elongation and straightening of the vessel takes place. Different abnormalities like undulations, kinks, and loops are due to the persistence of the embryological state of the vessel.9
Sometimes carotid elongation might be an acquired condition. Elongation of the adventitia occurs to a lesser extent as compared to its muscular wall. This disproportionate growth of the vessel layers is triggered by some pathological factors. That leads to the buckling or kinking of the vessels. This is exacerbated by atherosclerosis.10
Conclusion
The internal carotid artery was studied at its origin and course of the cervical part. The study arrived at the following conclusions:-
High origin of the ICA (38%) was found to be the commonest variation in the origin of the ICA, with a predisposition to the right side.
Commonest variation in the cervical part of ICA was kinking (32%), with a higher incidence on the left side.
A correlation was noted between the aberrant course and presence of kinks in the cervical part.
Aneurysm (4%) of the cervical part had equal predisposition to both sides, and had correlation with the presence of coiling of the vessel.
The relevance of this study was to create proper awareness about the variations in various parts of the ICA among the anatomists, as well as surgeons and radiologists, before performing interventional procedures. This would prevent diagnostic errors and help to avoid further complications.