Introduction
Female internal genital organs are derived from different embryological germ layers and are subjected to various congenital abnormalities, which are further complicated by hormonal axis.1
The uterus is a pear-shaped muscular organ in which the zygote after fertilization implants and advances into a mature embryo and then further develops into a fetus. The uterus is externally covered by peritoneum anterosuperiorly and is separated from the urinary bladder by the vesicouterine pouch. Posteriorly the uterine body and the supravaginal part of the cervix are separated from rectum by the recto-uterine pouch. The uterus is mobile organ and supported by various ligament.2
Besides its role in pregnancy and parturition, its significance is known in various medical conditions e.g., endometriosis, cancer of the endometrium, cervical dysplasia. Certain non-emergency conditions are always a subject of concern like fibroid or fibromyomas.3
Uterine fibroids are non-cancerous benign conditions composed of mass made of muscle and fibrous tissue.4 In about 40 percent of cases, a positive family history with a chromosomal abnormality (chromosome 6 or 7) and or the role of polypeptide growth factors-Epidermal growth factor (EGF), insulin-like growth factor-1 (IGF-1), transforming growth factor (TGF), may stimulate the growth of leiomyoma either directly or via estrogen effect.5
Approximately 1.6 million women are newly diagnosed with uterine fibroids each year in the United States. The latest update of NUFF-2010 says that 80% of all women is having fibroid in the United States.4 The condition is increased as more cases are identified and diagnosed.6 It is an essential medical condition as it is one of the causes of large numbers of hysterectomy, massive menstrual bleed, dysmenorrhea, dyspareunia, and post-partum bleeding throughout their life.3, 4
Case History
A 63 yrs. female patient, with lung cancer was donated under national body donor programme INC, for medical study and research. We identified parasitic fibroid or wandering fibroid which is a rare subserosal type.5
Material and Methods
During anatomy dissection of the cadaver, an abnormal connection was identified at the lower part of the greater omentum and in the pelvic cavity. After cutting the band, we found an abnormal fibromuscular tissue connected to the anterosuperior part of the fundus and the lower part of greater omentum.
After clear evaluation, uterus showed an irregular outline with following morphometry details:
Figure 1
Superior view of pelvic cavity showing relation of uterine parts and fibroid on the external surface. Fibromuscular band from anterosuperior part of uterus
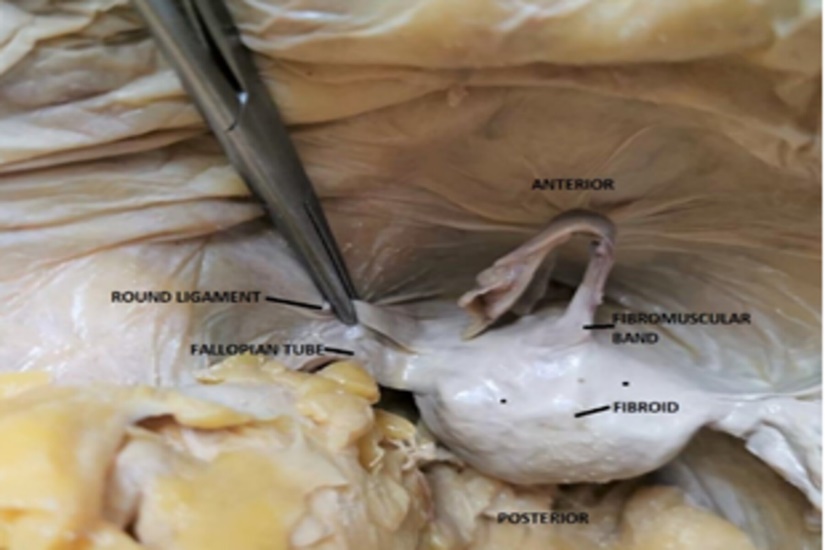
Externally uterus showed -multiple hard, nodular fibroids, with long fibromuscular band on the antero-superior part of the fundus. We did morphometry study of the fibroid band with following details:

Discussion
The uterus is derived from the paramesonephric duct (Mullerian duct), which arises as a longitudinal invagination of the epithelium on the anterolateral surface of the urogenital ridge. The cranial portions of the paramesonephric ducts develop into the uterine tube. The caudal portion forms the primordium. The primordia develops into the uterus, cervix, and superior 1/3rd of the vagina.1
Greater omentum covers the abdominal viscera and is derived from visceral peritoneum. Anatomically both uterus and greater omentum have different developmental origins.1 The uterus is supplied by the uterine artery, the uterine veins which drain into the uterovaginal venous plexus.1 The blood supply of greater omentum is from splanchnic vessels derived from gastroepiploic vessels from the celiac trunk. Congenital connection during fetal and later adolescent life is not reported due to their different developmental pathway.1, 2
Abnormal fistula like a bridge between the subserosal uterine fibroid and lower free margin of omentum are already reported previously. Parasitic fibroid is accidentally seen in abdominal surgeries,7 but immunohistology and radiological techniques can be used to diagnose the case.8, 9, 10
There is a very close relation in the anatomical position of the greater omentum, the fundus and posterior surface of the uterus.2, 11
However, in our case study, the parasitic fibroid band was seen on the anterior surface between fundus and body junction, where the possible explanation of pregnancy is guessed as it leads to change in anatomy to a more erect attitude of the uterus.5
The second possibility is a postoperative surgical complication wherein a patient is prone to develop parasitic fibroid after laparoscopic excision of fibroid.12
We did external morphometry study of the fibroid band without histology. However, in a recent study by Aron et al., histological changes in the form of fibromuscular overgrowth and collection of extracellular matrix are also reported.13
Conclusion
A parasitic fibroid is a rare but important complication of the uterine fibroid. Most of the cases are seen as an incidental finding. The postoperative adhesion of subserosal fibroid is the most common iatrogenic induced cause and may go unnoticed. Embryologically the development of greater omentum and uterus is different, but due to proximity of the two anatomical organs, the parasitic or wandering fibrous band get easy access to high nutrient areas like intestine or omentum. History of patients is valuable with possible use of higher investigation modality like MRI, immunohistology etc, for accurate diagnosis. Racial distribution, unexplained abdominal discomfort and unexplained menorrhagia in the history of patient could further help to achieve the diagnosis.