- Visibility 233 Views
- Downloads 38 Downloads
- Permissions
- DOI 10.18231/j.ijcap.2020.041
-
CrossMark

Abstract
Background: The vertebral column, sacrum, iliac bones and the lower limbs form a co-ordinated articular system with the two joints i.e., the hip joint and sacroiliac joint (SIJ). Our current understanding of biomechanics of this region is still quite inadequate, particularly with regard to multidirectional activities i.e. sports involving twisting and turning.
Materials and Methods: We have examined 160 normal adult hip bones. In each hip bone the outline of symphyseal, auricular and lunate acetabular surface area was marked on tracing paper. The surface area was then measured by digital planimeter.
Aim: An attempt has been made to correlate the various articular areas of hip bone and to find if any correlation exists between them applying Karl Pearson’s correlation coefficient formula.
Results: The average surface area of auricular surface for the two sides was 9.88cm2; that of lunate articular part of acetabulum 17.20cm2 and of pubis symphysis was found to be 2.60cm2. Further, differences between the two sexes have also been evaluated. In general, all the surface areas were found to be larger in males and more on the right side as compared to left.
Conclusion: There is a positive correlation seen between auricular and acetabular area; acetabular and symphyseal area and auricular and symphyseal area on both the sides. The findings of the present work can help in the better understanding of the normal kinematics of these joints and the resultant effects due to their dysfunction. Further it can help physiotherapists to properly plan out the treatment.
Introduction
During the changeover from the pronograde to the orthograde posture there has been a great change in the anatomy and functions of hip and pelvis as a whole. In terms of posture and locomotion, the pelvis is designed to support the downward and forward thrust transmitted to it by the weight of the trunk. Weight bearing and propulsive forces are also transmitted through the pelvis in reciprocal direction, as body weight is transferred alternately to each hip joint during gait.[1]
The weight from the fifth lumbar vertebrae (L5) is distributed equally along the alae of sacrum and through the ilium towards the acetabulum; the rest is transmitted across the horizontal ramus of the pubis and is counteracted at the symphysis pubis by a similar force from the opposite side. These lines of forces form a complete ring along the pelvic brim and there exists a complex system of bony trabeculae in the pelvic bones corresponding to these lines of force.[2] During evolution of erect posture of man, the weight of the body is transferred from the fifth lumbar vertebra to the base of the sacrum and thence through the acetabulum to the femoral head and ultimately to the lower limbs. The other concurrent change seen is that the ilia now lie vertically instead of horizontally (as in the the quadrupeds); sacrum being wedged between the two ilia, there is wider pelvis with acetabular cavities widely separated and the depth of the pubis is reduced.[1]
Regardless of the sports activity, normal function of the pelvis and hip is a prerequisite for normal athletic performance.[3] There is complete interdependence of the various elements of the pelvic brim so that any impairment at any level affects the structure as a whole and decreases the mechanical resistance. Palastanga et al. (2002) have estimated hip joint forces in normal subjects and stated that it ranged upto nearly six times body weight.[4]
The articular areas play a very important role in transmission of various forces including compression and reactionary forces, and also in the performance of various movements. The semilunar articular area of acetabulum is not equal in all places and in man it is widest where the head of femur is in maximum contact during erect posture and here the upper lip of acetabulum shows a general hypertrophy. This is located in the posterosuperior part (iliac) through which weight–cum–thrust bearing line passes and this area (the ‘dome’) is the widest and most extensive and it is narrowest in its pubic region.[5]
The articular surface of the ilium (auricular surface) lies on the posterosuperior part of medial aspect of hip bone. It is crescent shaped, concave posterosuperiorly. Its edges are well defined but the surface, though articular is rough and irregular. Its long axis contains a long crest lying between two furrows. This curved crest corresponds to an arc of circle whose centre lies approximately at the sacral tuberosity. This tuberosity is the point of insertion of the powerful sacroiliac ligaments. At the junction of the two segments of the iliac articular facet there is a slight elevation known as Bonnaire’s tubercle.[2]
The symphyseal surface is elongated and oval, covered by cartilage. The bony surface is irregular and shows small ridges and furrows or nodular elevations varying considerably with age and these features are of forensic value. At the pubis symphysis motion occurs vertically, with a shear type displacement of one pubic bone on the other, and in an anteroposterior rotational direction as one hemipelvis rotates forward on the other in gait (vertical motion-2 mm; rotatory movement-both in frontal and sagittal plane-generally less than 1.5mm).[3] The pubic symphysis is responsible for the integrity of pelvic ring.
The mechanics of pelvis does not lend itself to its critical analysis of complex movements. The variations described in the literature and seen in the specimens prompted us to measure the variations in size, length and shape of various articular facets of hip bone and to try and find if any correlation exists between these various facets.
Material and Methods
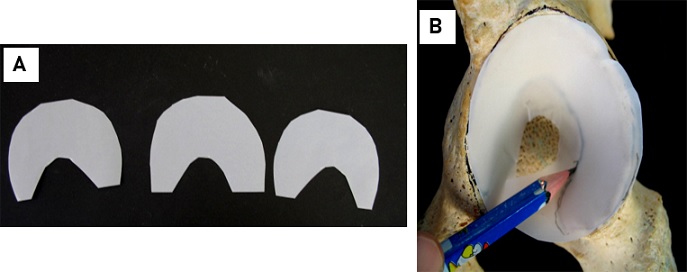
One hundred and sixty dry ([Table 1]), fully ossified apparently normal adult hip bones which did not show any congenital or pathological abnormalities, available in our department were utilized for this study. Side was determined by the two authors separately and side (right and left) was determined based on the external features of the bone. In each hip bone the outline of symphyseal, auricular and lunate acetabular surface areas were traced on tracing paper [[Figure 1], [Figure 2], [Figure 3]] and using digital planimeter KP-90N PLACOM (Lawrence and Mayo (India) pvt. Ltd. 274, Dr. D.N. Road, Mumbai -400001) [[Figure 4], [Figure 5]]. The surface areas were calculated separately for right and left side, as also for the male and female bones. The data so obtained was used to determine the correlation coefficient using Karl Pearson’s formula.
| Sex | Total | Right | Left |
| Male | 129 | 58 | 71 |
| Female | 31 | 15 | 16 |
| Total | 160 | 73 | 87 |
Results
As seen in [Table 2], the area of auricular surface in males was greater than in females on both the sides. The left auricular area in the male and right auricular area in female was greater. There was great variation observed in the size, shape and surface of auricular areas in the hip bones studied. The symphyseal articular area, which was mostly oval in outline, was greater in males on both sides as compared to females. In both male and female it was greater on right side. Acetabular surface area was distinctly greater in the males compared to females and it was greater on the right side in both sexes.
| Surface | Right | Left | ||
| Male | Female | Male | Female | |
| Auricular | 10.23 | 9.44 | 10.96 | 8.73 |
| Acetabular | 19.04 | 15.84 | 18.55 | 15.40 |
| Symphyseal | 2.46 | 2.42 | 2.38 | 1.96 |
| Total surface area cm2 | 31.73 | 27.70 | 31.89 | 26.09 |




Statistical analysis
The values of the various articular surface areas were used to find the Karl Pearson correlation efficient (r).[6]
As seen in [Table 3], acetabular lunate articular area was the largest articular area in all the bones examined of both sides and in both the sexes, contributing more than fifty percent of the surface area. The auricular area contributed approximately one third of the total surface area, whereas, symphyseal contribution was less than ten percent.
An attempt was made to establish correlation between auricular (A) & symphyseal (B) [AB(r)]; auricular (A) & acetabular (C) [AC(r)] and symphyseal (B) & acetabular (C) suface area [BC(r)]as shown in [Table 4]. All the values of ‘r’ were less than 1.00.
| Surface | Right | Left | Average | ||
| Male | Female | Male | Female | ||
| Auricular | 32.28 | 32.28 | 34.36 | 33.46 | 33.03 |
| Acetabular | 60.08 | 57.10 | 59.02 | 59.03 | 58.80 |
| Symphyseal | 7.63 | 8.86 | 7.52 | 7.51 | 7.88 |
| Correlation | Right | Left | ||
| Male | Female | Male | Female | |
| AB (r) = | 0.87 | 0.88 | 0.89 | 0.78 |
| AC (r) = | 0.95 | 0.92 | 0.93 | 0.94 |
| BC (r) = | 0.92 | 0.87 | 0.98 | 0.78 |
Discussion
For more than a century the type and movements at the sacroiliac joints (SIJs) had been shrouded in mystery. It is an enigmatic joint. The controversy has raged for centuries, most significantly in its classification, cartilage type, innervation, propensity for movement, and predilection for causing pain. Schafer et al. (1987) have stated that like fingerprints, their exact design is unique to the individual.[7] Interest in these joints was generated first by obstetricians. Attention devoted to them as a primary source of mechanical dysfunction and pain has waxed and wanned. The SIJs especially fell into disfavor as producers of pain when key role of the Inter Vertebral Disc (IVD) in back pain gained ground. It is capable of limited motion and therefore subject to mechanical dysfunction. Antagonists of these arguments contend that motion at these joints is nearly impossible, considering the complexity of its topography, the magnitude of force required for its disruption, the referred nature of the pain attributed to it, and the flawed nature of the analysis of its motion. Earlier the SIJ was classified variably as a cartilaginous joint (amphiarthrosis), a synchondrosis that is ultimately replaced by bone, a diarthroamphiarthrodial joint, a cross between a synarthrosis and diarthrosis. Some concluded that the joint is synovial (diarthrodial) but becomes an amphiarthrosis under certain pathological conditions. The trend today is to include both the iliac and sacral auricular surfaces and tuberosities in the make-up of the SIJ. The auricular surfaces form a synovial joint and the tuberosities connected by an interosseous ligament constitute fibrous form of a synarthrosis. Although the synovial part of the joint is usually classified as plane, accessory SIJ articulations are formed frequently from posteriorly positioned supernumery articular facets.[8]
Anteroinferiorly auricular surfaces are complementary L shaped surfaces, while the tuberosities are paired irregular pitted areas positioned posterosuperior to the auricular surfaces. The tuberosities are connected by massive interosseous sacroiliac ligament. The ‘L’ shaped auricular surfaces have two limbs that point posteriorly and embrace a dorsal concavity. The shorter more vertically oriented cephalic limb consists of the first segment on the sacral side, while the caudal limb is longer, more horizontal, and composed of the second and third segments on the sacral side. The auricular surfaces are strikingly variable however, both between subjects and from side to side within the same subject. Shapes include C or L shape and limbs may be short or long which may be equal or unequal. The angle formed between the two limbs is obtuse or perpendicular. The overall orientation of the joint is obliquely vertical, making it the only weight bearing joint that is not transverse to the transfer of weight.[8]
The ilium significantly antedates the sacrum in development. Joint cavitation, which is complete by 12 weeks begins later and progresses more slowly in the SIJ. A joint cavity appears by 7th week and reaches its full extent in 7th or 8th month; a joint capsule is lined by synovial membrane at 37th week. At birth the joint surfaces are flat and smooth, and the capsule is thin and pliable. During the first 10 years, the auricular surfaces remain flat and permit gliding motions in all directions. In the teen years, the complementary unevenness starts to develop on two auricular surfaces. By early twenties, a convex iliac ridge and a concave sacral depression have formed and run centrally along the length of the joint surface. The congruency of the opposite joint surfaces is usually high; eminences are more frequent on the ilium, and ‘almost every conceivable combination of grooves, ridges, eminences and depressions’ is apparent. Auricular surfaces of female are smaller and flatter than those in females. In the middle of the third decade, surfaces begin to show signs of degeneration. Joint degeneration progresses from the fourth through the eighth decade. The degenerative changes that develop on the iliac side appear first and are more severe than those on the sacral side.[8]
Acetabulum is not always of the same shape, width, or depth. Minor anatomical abnormalities in the acetabular shape and joint congruences are frequent which may have some bearing on the acetabular reconstruction and femoro-acetabular impingement. Acetabular fossa may have an irregular cloverleaf shape.
Pal (1989) measured the surface areas of body of sacrum, superior articular facets and the mean surface area of two auricular surfaces and found a significantly high correlation between the vertebral and iliac areas. The value given by Pal for the two auricular surfaces (18.4 +/- 2.19 cm2) is comparable if we add up the surface areas of the auricular surfaces in the male (21.19 cm2) and in the female (18.17 cm2).[9]
Anatomical knowledge of the articular surfaces if hip joint is of utmost importance to orthopaedic surgeons as articular surface injuries are a significant problem for which current treatments is uncertain. They are common and many of these injuries initiate progressive joint degeneration, considered as post-traumatic osteoarthritis. Risk of post-traumatic osteoarthritis can be reduced by surgeons efforts by restoring joint stability, congruity, and alignment following injury. Surgeons also use periosteal and perichondral grafts and autologous chondrocytes to promote repair and remodeling of damaged articular surfaces.[10] Still researches are going on that would help to maintain chondrocyte viability and function, restore joint stability and congruity, and promote articular surface repair and remodeling following joint injury.
Conclusion
The findings of our study can help in the better understanding of the normal kinematics of various joints of hip bone and the resultant effects due to their dysfunction. No work of similar nature has been carried out earlier and hence the findings of the present work can not be compared with any other work and prior to this, no attempt has been made to find the correlation coefficient between the various articular surfaces of hip bone. The present findings may be of value to orthopedic surgeons and physiotherapists in designing and planning of therapy for low backache, and SIJ dysfunction.
Source of Funding
None.
Conflict of Interest
None
References
- Taher SA, Ayer AA. Weight bearing line in the acetabulum and its evolutionary significance. J Anat Soc Ind. 1962;XI(1):9-14. [Google Scholar]
- Kapandaji IA. The Physiology of Joints. Vol. 3, In Trunk and Vertebral Column. Trunk and Vertebral Column. 1995;3:56-9. [Google Scholar]
- Zuluaga M, Briggs C, Carlisle C, Mcdonalds V, Mcmeeken J, Nickson W, et al. . Sports Physiotherapy, Applied Science and Practice: In the pelvis, hip and thigh. 1995. [Google Scholar]
- Palastanga N, Field D, Soames R. . Anatomy and Human Movement: structure and function, 4th Edn. 2002. [Google Scholar]
- Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dusse KJE. . Gray’s Anatomy: The Anatomical basis of Medicine and Surgery. 38th Edn. 1995. [Google Scholar]
- Mahajan BK. . Methods in Biostatistics: For Medical Students and Research Workers, 6th Edn. 1997. [Google Scholar]
- Schafer RC. . Clinical Biomechanics: Musculoskeletal Actions and Reactions. 2nd Edn. 1987. [Google Scholar]
- Oatis CA. . Kinesiology: The Mechanics and Pathomechanics of Human Movement. 2004. [Google Scholar]
- Pal G. Weight transmission through the sacrum in man. J Anat. 1989;162:9-10. [Google Scholar]
- Buckwalter JA, Marsh JL, Brown T, Amendola A, Martin JA. Principles of Tissue Engineering. Articular Cartilage Injury. 4th Edi. ;2014:1253-66. [Google Scholar]