Introduction
Middle cardiac vein commences at the apex of the heart and ascends along the posterior interventricular groove toward the coronary sinus. It runs in the posterior interventricular groove to end in the coronary sinus near its atrial end. It drains the posterior aspect of left and right ventricles and the interventricular septum. It then joins the coronary sinus within the millimeters of the sinus entering into the right atrium.1, 2, 3
Cardiac venous system was a neglected field however it has now begun to attract more attention with development of new interventional techniques such as coronary catheterization and selective catheterization of the cardiac veins. As MCV is one of the constant tributaries of coronary sinus. Middle cardiac vein may be one of the choices of implantation of pacing leads. Middle cardiac vein did not generate any variations due to its short course before draining into the right atrium therefore middle cardiac vein can provide an important alternate route for ventricular defibrillation.4
Therefore, clinical significance of middle cardiac vein prompted us to undertake a detailed study of middle cardiac vein to know more about its morphology and its significant value in the designing of surgical devices. Such type of studies is less in Indian scenario; therefore, this study provides dimensions of middle cardiac vein (e.g. length, diameter) for interventional procedures in India. So, their understanding will allow for future medical devices to be engineered successfully for delivering therapies to a variety of patients.
Materials and Methods
The present study was conducted on the 30 human hearts of different age group (varies from 15-65 years) from embalmed cadavers of the Department of Anatomy, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly during a period of two years (2012-2013). The weight of cadavers was recorded. The hearts were washed gently to remove any blood clots, if any. The human hearts were fixed in 10 % formalin and dissected. The morphology of middle cardiac vein in human hearts was observed. The length and diameter of middle cardiac vein was measured with the help of digital Vernier calipers. Relation of length of middle cardiac vein, with posterior interventricular artery was observed.
Observation and Results
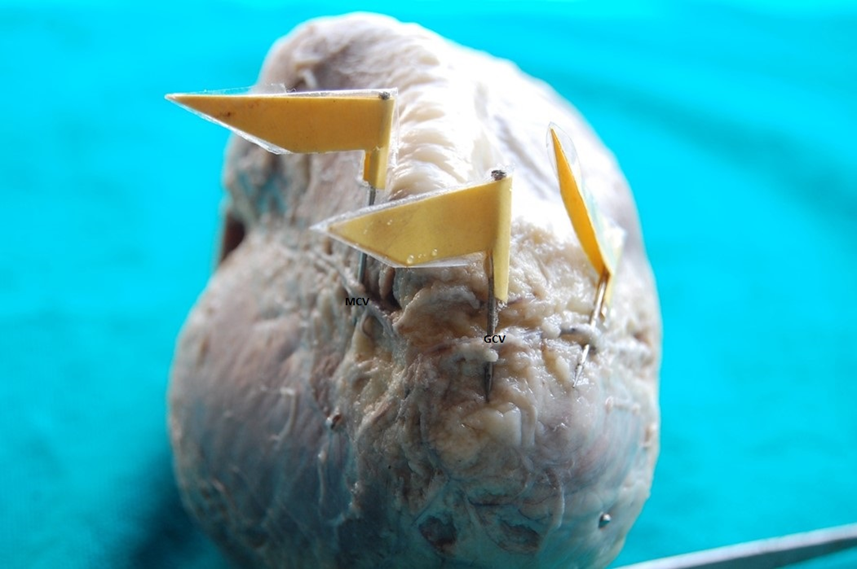
The present study revealed that Middle cardiac vein is present in all hearts. The mean diameter of middle cardiac vein is 2.57+1.16 mm and the mean length of MCV is 74.69+21.10 mm. (Figure 1) It was also found that in two hearts MCV reaches up to apex of heart (6.66%) (Figure 2). MCV was tortuous in one heart (3.33%) while in rest of the hearts MCV was straight. We also observed statistically significant relationship between length of MCV and weight of cadaver (50-70 kg) (r = 0.36, p value = 0.031) (Table 1). In our study, we measured the length of the MCV (75.94 +/-20.32 mm) in cadaveric hearts. There was no significant relation between age of cadaver and length of MCV (r=0.029, p value=o.875). The diameter of middle cardiac vein as far as statistical analysis is concern shows no significant relation with age (coefficient of correlation- 0.24, p value- 0.197) (Table.1).
Table 1
Table 1: Showing length and diameter of middle cardiac vein (MCV)
Figure 1
Showing measurement of diameter of middle cardiac vein with the help of digital Vernier calipers
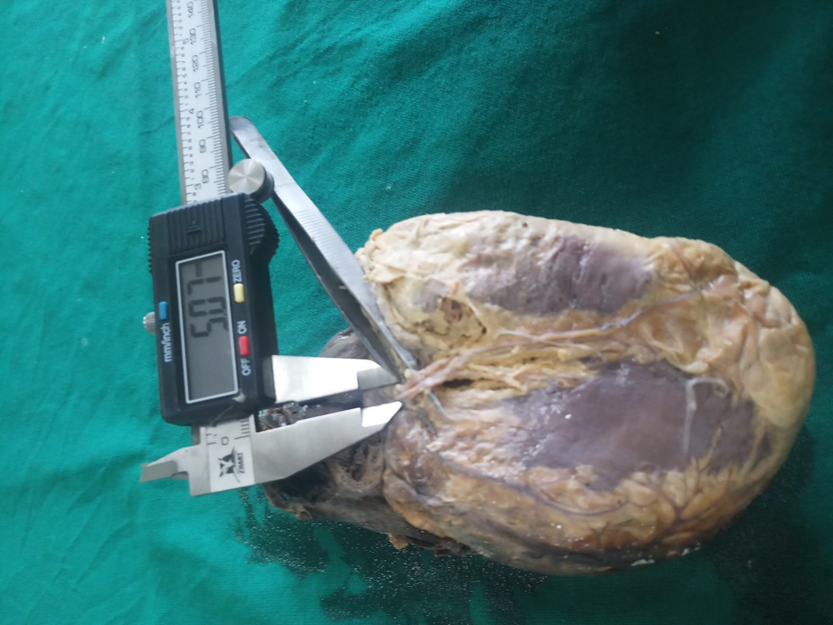


Figure 4
Common trunk* form by small cardiac vein**, accessory middle cardiac vein*** & middle cardiac vein****.

The two tributaries of MCV were enclosing posterior interventricular artery, after that they join each other and drain into coronary sinus (Figure 3) (3.33%). In eight hearts the MCV and SCV together form common trunk and drain into coronary sinus (26.66%) (Figure 4). In one heart, we found presence of accessory middle cardiac vein (3.33%) and it forms common trunk with middle cardiac vein and small cardiac vein (Figure 4).
In our study we witnessed the anastomoses (Figure 5) in between anterior interventricular artery & middle cardiac vein in five hearts (16.66%) and the anastomoses between GCV & MCV in eleven hearts (36.66%) that means in our study the total 16 cadaveric hearts (53.33%) presented the anastomoses. It was also observed that the anastomoses were present at the apex of heart.
Table 2
Comparison of diameter of middle cardiac vein from present study with others as reported in literature
Discussion
In the present study the morphology of MCV have been observed and various parameters of MCV have been taken.
Joseph B. Goldsmith and H. W. Butler11 observed pig embryos of closely graded series of 2 mm to over 300 mm in length. They found that middle cardiac vein is the first cardiac vein in 9 mm embryo arises from the ventricular border of the coronary sinus, slightly to the left of the opening of the sinus into the sinus venosus. This vein arises as an endothelial bud from the inner walls of the coronary sinus and extends through the connective tissue of the atrio-ventricular groove toward the posterior interventricular groove.
In our study we observed anastomoses in 16 cadaveric hearts (53.33%) out of 30 hearts at the apex of heart. These anastomoses were present in between artery and vein i.e. anterior interventricular artery & middle cardiac vein in 5 hearts (16.66%) and in between great cardiac vein and middle cardiac vein in 11 hearts out of 30 (36.66%). Ortale J R et al12 observed that an anastomosis of approximately 1.0 mm caliber was observed between the anterior and posterior interventricular veins in 19 % of specimens. Pejkovic B and Kranjc I.6 found arteriovenous anastomoses in 6 % of the cases. Luis E Ballestereos5 reported that anastomosis of the great and middle cardiac veins was present in 58.8%; 33.8% in the heart apex and in the anterior interventricular sulcus.
Maric I13 found in two cases a common trunk of small cardiac vein and the middle cardiac vein which opened into the coronary sinus. In our study, we also observed small cardiac vein and middle cardiac vein together form common trunk which opens into coronary sinus.
Abdel Meguid14 observed that in two cases that the SCV joined MCV to form the common trunk which opened into the CS, in one specimen they observed two parallel MCV ran in the posterior interventricular groove. In our study middle cardiac vein is also constantly present tributary of coronary sinus. We also found that SCV joined MCV to form the common trunk which opened into the CS, in one heart we observed two parallel MCV ran in the posterior interventricular groove.
B Pejkovic6 found that MCV was tributary of CS in 92% hearts or it entered directly into the right atrium (8%). In our study middle cardiac vein is also constantly present tributary of coronary sinus.
Liu Xianxia7 reported that the consistently presence of MCV is alone in almost all patients but in only one patient it was double. We also observed middle cardiac vein is constant tributary of coronary sinus, and in one heart we observed two parallel MCV ran in the posterior interventricular groove.
Genc B15 found that a dual middle cardiac vein was present in nine of the 339 patients (2.6%).9, 7 They also observed that in 29.2% (19/65) of small cardiac vein drained directly into the middle cardiac vein. In our study, we observed in one heart that two parallel MCV ran in the posterior interventricular groove. We also found that SCV joined MCV to form the common trunk which opened into the CS.
Gilard M10 and Qinzhu W9 also observed that the middle cardiac vein is present in all hearts. We also find MCV is present in all hearts.
Conclusion
The dimensions of middle cardiac vein can be used for radiofrequency ablation of a posteroseptal accessory pathway and for new interventional technique such as selective catherization of middle cardiac vein. The dimensions of middle cardiac vein may provide one of the choices of implantation of pacing leads.