Introduction
The occipital condyle is an important part of the craniovertebral junction and the articulation between the occiput and atlas. Occipital condyles are important element to maintain the head vertically. The integrity of the atlanto-occipital joint is of vital importance for the stability of the craniovertebral junction.1 The stability of this craniovertebral junction depends largely on the morphometric data of the occipital condyles.2 Occipital plates are commonly used as the cephalad fixation point in these constructs but issues such as the need for multiple points of fixation within a limited area, limited surface area for grafting and potential for intracranial injuries have led to investigations for alternatives.3 There are many kinds of pathological processes that involve the cranio vertebral junction. These lesions include intradural tumours such as meningiomas, neurinomas or vascular
lesions such as aneurysms and arteriovenous malformations of the vertebral artery and vertebrobasilar junction, extradural tumours such as chordomas, basilar invagination and other congenital anomalies, nontraumatic (rheumatoid) and traumatic entities with C1 — C2 subluxation.4 The distance between anatomic landmarks and the sites where a number of vital structures have their entrance or exit are very important for clinical application, therefore the assessment of morhometry of occipital condyles and foramen magnum is helpful for lateral surgical approach for reaching lesion in the middle and posterior part of cranial base. So the study of morphometric analysis of occipital condyles and foramen magnum has been undertaken with view to be helpful particularly to the neurosurgeons, radiologists and orthopedicians in preoperative process.
Materials and Methods
After obtaining permission of Institutional Review Board the study has been done. The material for the present study consists of 150 dry skulls of unknown sex. These were collected from Govt. Medical College, Bhavnagar, P.D.U Medical College, Rajkot, GMERS Medical College, Valsad and K.J.Mehta Medical College, Amargadh, Bhavnagar.
Morphometric methods: - All measurements were recorded using a digital vernier caliper. Measurements were taken using below mentioned bony landmarks on the skull,
Anterior midpoint of foramen magnum (basion)
Posterior midpoint of foramen magnum (opisthion)
Anterior tip of right occipital condyle
Posterior tip of right occipital condyle
Anterior tip of left occipital condyle
Posterior tip of left occipital condyle
Following parameters were recorded:-
a. The length of occipital condyle: distance from its anterior tip to posterior tip
b. Width of the occipital condyle: maximum distance measured at the right angles to the line joining its anterior and posterior tips
c. Height of the occipital condyle: thickness of the condyle on the centre of the occipital condyle
d. Anterior intercondylar distance: distance between the anterior tips of right and left condyles
e. Posterior intercondylar distance: distance between the posterior tips of right and left condyles
f. Distance between basion and anterior tip
g. Distance between basion and posterior tip
h. Distance between opisthion and anterior tip
i. Distance between opisthion and posterior tip
j. Anteroposterior diameter of foramen magnum
k. Location of intracranial orifice of right hypoglossal canal
l. Location of intracranial orifice of left hypoglossal canal
m. Location of extracranial orifice of right hypoglossal canal
n. Location of extracranial orifice of left hypoglossal canal
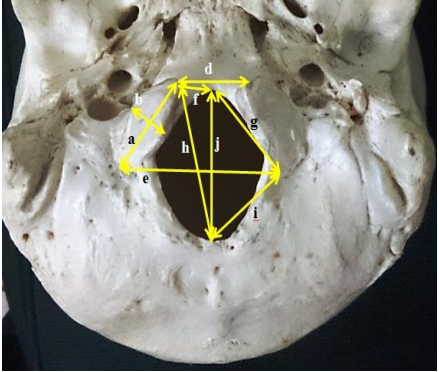
Table 1
Show location of intracranial and extracranial orifices of hypoglossal canal

Results
The total of 150 skulls was studied. The data was analyzed by and statistical analysis was carried out and the results have been tabulated.
Table 2
Show results of different paprameters
Table 3
| Location | Intracranial orifice | Extracranial orifice | ||
| Right (%) | Left (%) | Right (%) | Left (%) | |
| 1 | 0.67 | 0.67 | 88 | 88 |
| 2 | 4 | 4 | 43 | 43 |
| 3 | 18.67 | 20 | 12 | 12 |
| 4 | 50.66 | 49.33 | 4 | 4 |
| 5 | 16.67 | 18 | 3 | 3 |
| 6 | 9.33 | 8 | - | - |
| 7 | 0 | 0 | - | - |
Show intracranial and extracranialorifices of hypoglossal canal
Table 4
| Mean (mm) | Standard deviation (SD) | |
| Anterior intercondylar distance | 18.80 | 3.30 |
| Posterior intercondylar distance | 44.56 | 4.5 |
Show mean anterior and posterior intercondylar distance
The occipital condyles were also classified according to their length. The condyle less than 20mm was called Type-1 (short), the condyle length in range of 20–26mm was called Type-2 (moderate) and the condyle more than 26mm was called Type-3 (long).
Discussion
In the present study mean anterior intercondylar distance of 150 skulls is found to be 18.80mm and SD is 3.30 and posterior intercondylar distance of 150 skulls is found to be 44.56mm and SD is 4.5. There is significant difference between anterior and posterior intercondylar distance. This difference reflects the asymmetry in orientation of occipital condyles which may affect lateral approach. According to recent studies condylectomy provides the wider angle of exposure. Occipital condyle forms lateral limit of cranio-vertebral junction. The configuration and orientation of occipital condyles may affect lateral approach. Most Of the approaches necessitate resection of occipital condyle, partially or completely. Long occipital condyle may require extensive resection for optimum visualization.
In the present study, mean length of right occipital condyle in 150 skulls is 23.97mm and SD is 2.31 and mean length of left occipital condyle is 23.36mm and SD is 2.84. Significant difference was found in right and left occipital condylar length as shown by result of student T test (p=0.0440).
Also the classification of occipital condyle according to its length is carried out, where type – 1 occipital condyle (short < 20mm) are found in 2% and 8.67% in right and left side respectively, type – 2 occipital condyle (moderate 20 – 26mm long) are found in 77.33% and 73.33% in right and left side respectively, type – 3 (long > 26mm) are found in 20.67% and 18% in right and left side respectively. Naderi et al reported to be short in 8.6%, moderate in 77.2% and long in 14.1%.1
Mean condylar width is found to be 12.27mm and SD is 2.07 in right OC & 12.57mm and SD is 2.38 in left OC. No significant difference was found in width between right and left OC as shown by student t test (p=0.243). The length and width of the occipital condyle were also assessed radiologically by some authors. In the present study mean codylar length is reported to be 23.97mm and 23.36mm in right and left occipital condyle respectively, in radiological study, reported by Murshad et5 al it was found to be 24.38mm and 24.00mm which is more than the present study.
Condylar height is found to be 9.26mm and SD is 1.67 in right OC and 9.09mm and SD is 1.52 in left occipital condyle. No significant difference is found in height between right and left OC as shown by student T test (p=0.380).
The distance between the anterior tip of OC and the basion is measured 9.20mm and 9.54mm in right and left condyles respectively, while Naderi et al reported them to be 10.5mm and 11.1mm.1 The distance between posterior tip of OC and the basion is 28.07mm and 28.12mm in right and left condyles respectively, which is very near to the result obtained by Naderi et al who reported it to be 28mm.1
The distance between anterior tip of occipital condyle and opisthion is measured 38.03mm and 37.93mm in right and left OC respectively, while Naderi et al reported them to be 38.9mm and 39.1mm. The distance between posterior tip of occipital condyle and opisthion is 28.68mm and 28.27mm in right and left OC respectively. The distance between the posterior tip of OC and opisthion is also an important anatomical factor. The larger the distance, the free the space for the posterolateral approach.
Mormphometric data of occipital condyles is useful to evaluate the safer transcondylar approach for craniovertebral surgery. The intracranial orifice (ICO) of HC is located medial to the Occipital Condyle. In the present study intracranial orifice is found to locate principally at location 3 and 4. No orifice was found in location 7. As the resection of the OC depends on intracranial orifice of HC, so this posterior one fourth with location 7 can be resected safely. Drilling of the OC can be performed after reaching the lateral aspect of the intracranial end of HC because the canal is directed anteriorly and laterally permitting the lateral portion of posterior 2/3rd of condyl e to be removed without entering the HC.1,2
Conclusion
It can be concluded that careful radiological a nalysis of occipital condyles is required before craniovertebral junction surgery to prevent injury to structure passing through foramen magnum. Also the posterior quadrant do not possess the intracranial orifice of hypoglossal canal in relation to occipital condyle, it is the safer site for surgical approach.